

Morbid obesity may increase dislocation in total hip patients: a biomechanical analysis
- PMID: 22907474
- PMCID: PMC3563777
- DOI: 10.1007/s11999-012-2512-3
Morbid obesity may increase dislocation in total hip patients: a biomechanical analysis
Abstract
Background: Obesity has reached epidemic proportions in the United States. Recently, obesity, especially morbid obesity, has been linked to increased rates of dislocation after THA. The reasons are unclear. Soft tissue engagement caused by increased thigh girth has been proposed as a possible mechanism for decreased joint stability.
Questions/purposes: We asked (1) whether thigh soft tissue impingement could decrease THA stability, and if so, at what level of BMI this effect might become evident; and (2) how THA construct factors (eg, head size, neck offset, cup abduction) might affect stability in the morbidly obese.
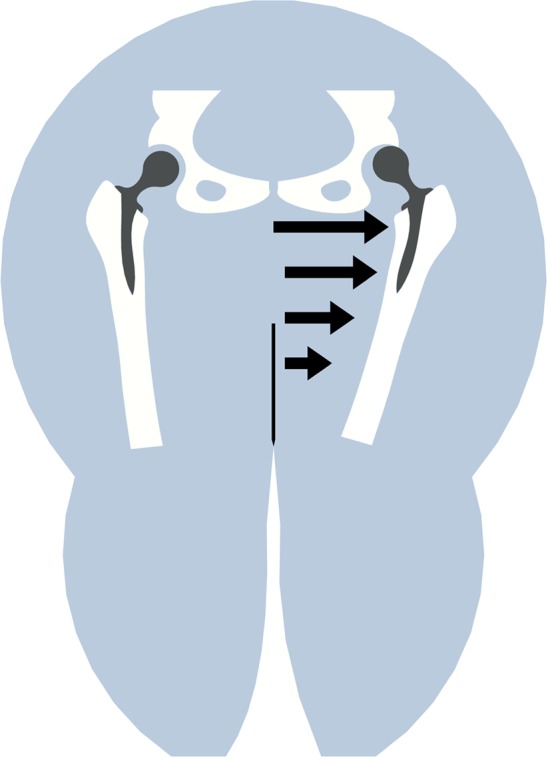
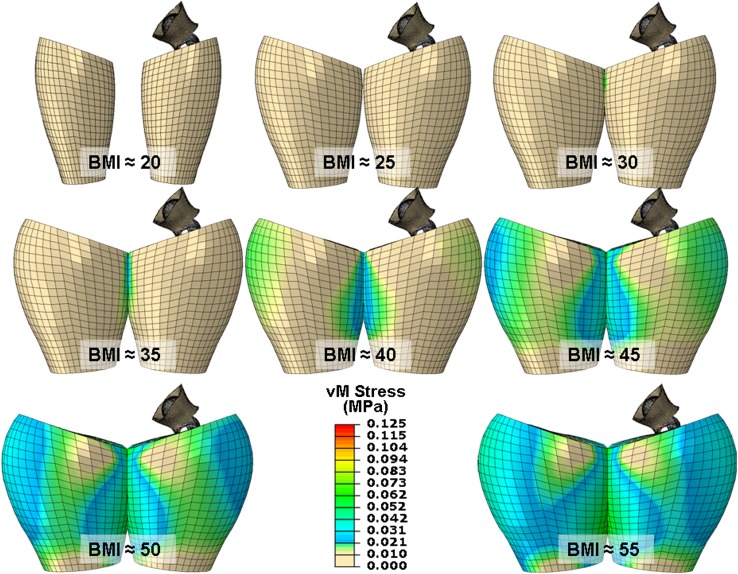
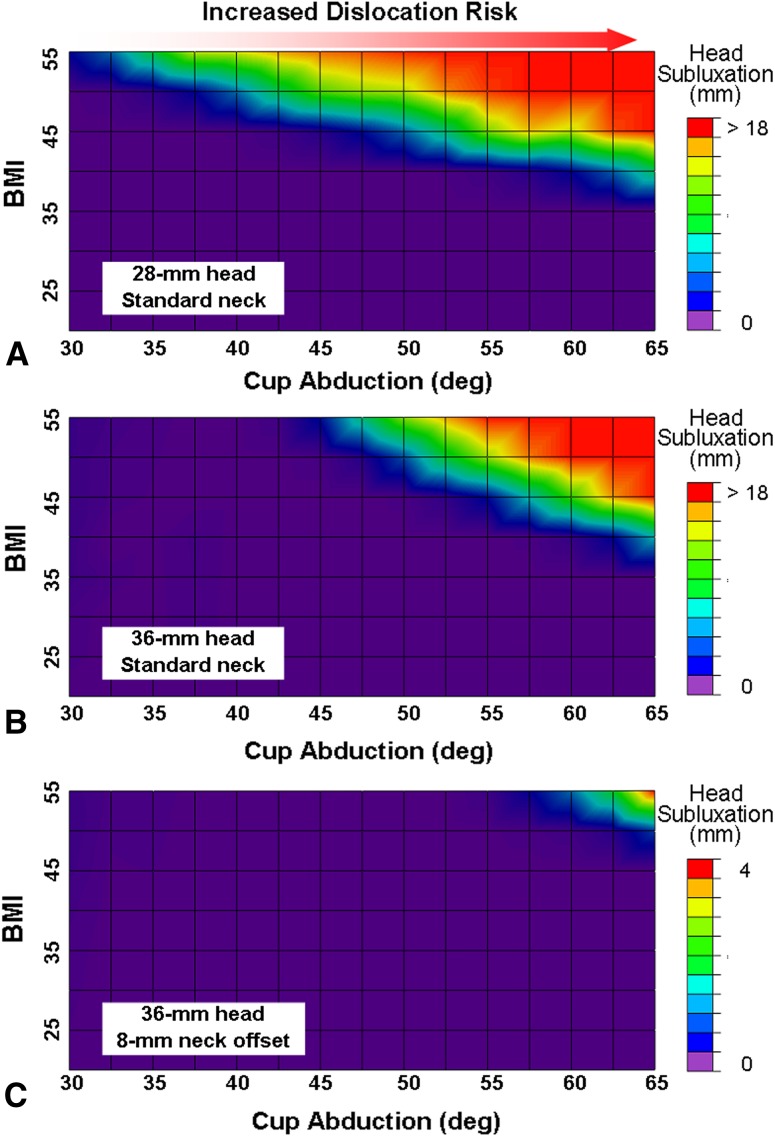
Methods: The obesity effect was explored by augmenting a physically validated finite element model of a total hip construct previously comprising just implant hardware and periarticular (capsular) soft tissue. The model augmentation involved using anatomic and anthropometric data to include graded levels of increased thigh girth. Parametric computations were run to assess joint stability for two head sizes (28 and 36 mm), for normal versus high neck offset, and for multiple cup abduction angles.
Results: Thigh soft tissue impingement lowered the resistance to dislocation for BMIs of 40 or greater. Dislocation risk increased monotonically above this threshold as a function of cup abduction angle, independent of hardware impingement events. Increased head diameter did not substantially improve joint stability. High-offset necks decreased the dislocation risk.
Conclusions: Excessive obesity creates conditions that compromise stability of THAs. Given such conditions, our model suggests reduced cup abduction, high neck offset, and full-cup coverage would reduce the risks of dislocation events.
Figures






References
-
- Aritan S, Oyadiji SO, Bartlett RM. The in vivo mechanical properties of muscular bulk tissue. Conf Proc IEEE Eng Med Biol Soc. 2009;2009:5259–5262. - PubMed
-
- Barrack RL. Dislocation after total hip arthroplasty: implant design and orientation. J Am Acad Orthop Surg. 2003;11:89–99. - PubMed
-
- Bartz RL, Noble PC, Kadakia NR, Tullos HS. The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am. 2000;82:1300–1307. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
