

The Joint Commission Children's Asthma Care quality measures and asthma readmissions
- PMID: 22908110
- PMCID: PMC4074621
- DOI: 10.1542/peds.2011-3318
The Joint Commission Children's Asthma Care quality measures and asthma readmissions
Abstract
Background and objectives: The Joint Commission introduced 3 Children's Asthma Care (CAC 1-3) measures to improve the quality of pediatric inpatient asthma care. Validity of the commission's measures has not yet been demonstrated. The objectives of this quality improvement study were to examine changes in provider compliance with CAC 1-3 and associated asthma hospitalization outcomes after full implementation of an asthma care process model (CPM).
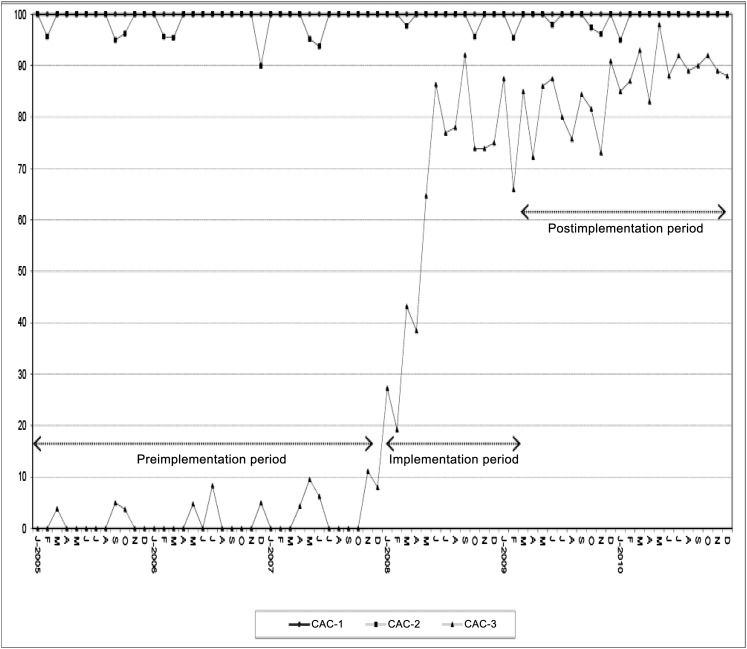
Methods: The study included children aged 2 to 17 years who were admitted to a tertiary care children's hospital for acute asthma between January 1, 2005, and December 31, 2010. The study was divided into 3 periods: preimplementation (January 1, 2005-December 31, 2007), implementation (January 1, 2008-March 31, 2009), and postimplementation (April 1, 2009-December 31, 2010) periods. Changes in provider compliance with CAC 1-3 and associated changes in hospitalization outcomes (length of stay, costs, PICU transfer, deaths, and asthma readmissions within 6 months) were measured. Logistic regression was used to control for age, gender, race, insurance type, and time.
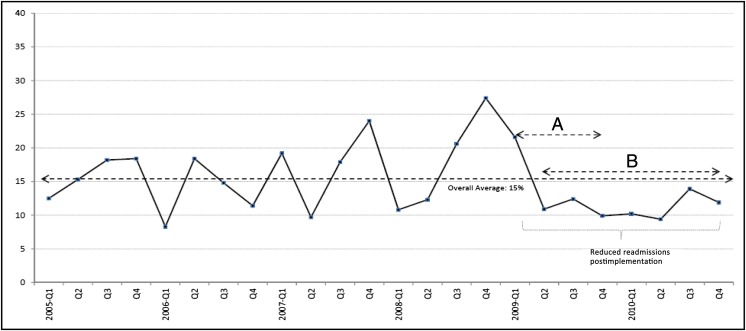
Results: A total of 1865 children were included. Compliance with quality measures before and after the CPM implementation was as follows: 99% versus 100%, CAC-1; 100% versus 100%, CAC-2; and 0% versus 87%, CAC-3 (P < .01). Increased compliance with CAC-3 was associated with a sustained decrease in readmissions from an average of 17% to 12% (P = .01) postimplementation. No change in other outcomes was observed.
Conclusions: Implementation of the asthma CPM was associated with improved compliance with CAC-3 and with a delayed, yet significant and sustained decrease in hospital asthma readmission rates, validating CAC-3 as a quality measure. Due to high baseline compliance, CAC-1 and CAC-2 are of questionable value as quality measures.
Figures
References
-
- Guide for State Health Agencies in the Development of Asthma Programs; US Department of Health and Human Services, Centers for Disease Control and Prevention. CDC. Asthma prevalence, health care use and mortality, 2000-2001. Available at: www.cdc.gov/nchs/products/pubs/pubd/hestats/asthma/asthma.htm. Accessed February 26, 2010
-
- Akinbami LJ, Schoendorf KC. Trends in childhood asthma: prevalence, health care utilization, and mortality. Pediatrics. 2002;110(2 pt 1):315–322 - PubMed
-
- Fuhlbrigge AL, Adams RJ, Guilbert TW., The burden of asthma in the United States Am J Respir Crit Care. 2002;166(8):1044–1049 - PubMed
-
- Nkoy FL, Fassl BA, Simon TD, et al. . Quality of care for children hospitalized with asthma. Pediatrics. 2008;122(5):1055–1063 - PubMed
-
- Friday GA, Jr, Khine H, Lin MS, Caliguiri LA. Profile of children requiring emergency treatment for asthma. Ann Allergy Asthma Immunol. 1997;78(2):221–224 - PubMed
Publication types
MeSH terms
Grants and funding
- K23 HD052553/HD/NICHD NIH HHS/United States
- K23 NS062900/NS/NINDS NIH HHS/United States
- R18 HS018678/HS/AHRQ HHS/United States
- KM1 CA156723/CA/NCI NIH HHS/United States
- 1R18HS018678-01A1/HS/AHRQ HHS/United States
- UL1 RR025014/RR/NCRR NIH HHS/United States
- K23 HD052553-01A1/HD/NICHD NIH HHS/United States
- KM1CA156723/CA/NCI NIH HHS/United States
- 1R18HS018166-01A1/HS/AHRQ HHS/United States
- K23NS062900/NS/NINDS NIH HHS/United States
- R18 HS018166/HS/AHRQ HHS/United States
- ULI RR025014/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
