

Racial/ethnic differences in infant mortality attributable to birth defects by gestational age
- PMID: 22908111
- PMCID: PMC4605418
- DOI: 10.1542/peds.2011-3475
Racial/ethnic differences in infant mortality attributable to birth defects by gestational age
Abstract
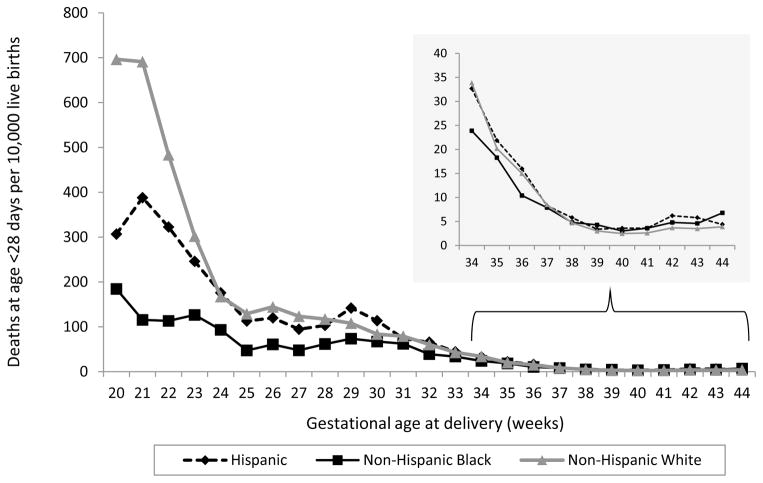
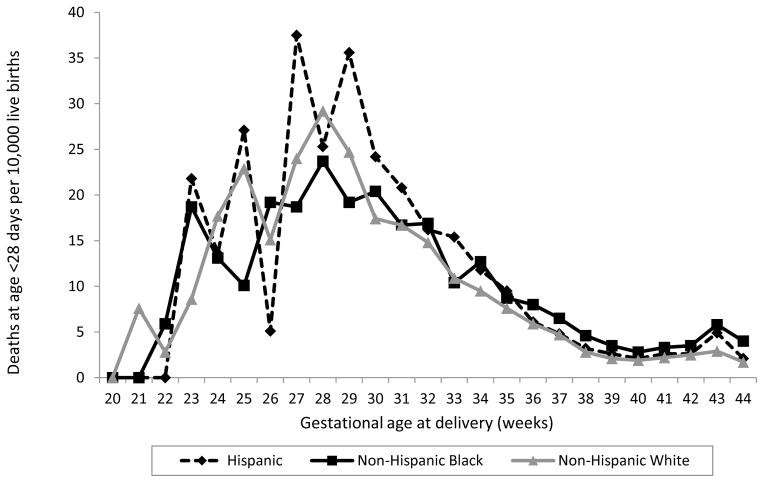
Objective: Birth defects are a leading cause of infant mortality in the United States. Previous reports have highlighted black-white differences in overall infant mortality and infant mortality attributable to birth defects (IMBD). We evaluated the impact of gestational age on US racial/ethnic differences in IMBD.
Methods: We estimated the rate of IMBD as the underlying cause of death using the period-linked birth/infant death data for US residents for January 2003 to December 2006. We excluded infants with missing gestational age, implausible values based on Alexander's index of birth weight for gestational age norms, or gestational ages <20 weeks or >44 weeks; we categorized gestational age into 3 groups: 20 to 33, 34 to 36, and 37 to 44 weeks. Using Poisson regression, we compared neonatal and postneonatal IMBD for infants of non-Hispanic black and Hispanic mothers with that for infants of non-Hispanic white mothers stratified by gestational age.
Results: IMBD occurred in 12.2 per 10 000 live births. Among infants delivered at 37 to 44 weeks, blacks (and Hispanics, to a lesser degree) had significantly higher neonatal and postneonatal IMBD than whites; however, among infants delivered at 20 to 33 or 34 to 36 weeks, neonatal (but not postneonatal) IMBD was significantly lower among blacks compared with whites.
Conclusions: Racial/ethnic differences in IMBD were not explained in these data by differences in gestational age. Further investigation should include an assessment of possible racial/ethnic differences in severity and/or access to timely diagnosis and management of birth defects.
Conflict of interest statement
Conflicts of interest: None.
Figures
References
-
- CDC. Update on overall prevalence of major birth defects—Atlanta, Georgia, 1978–2005. MMWR Morb Mortal Wkly Rep. 2008;57:1–5. - PubMed
-
- Petrini J, Damus K, Russell R, Poschman K, Davidoff MJ, Mattison D. Contribution of birth defects to infant mortality in the United States. Teratology. 2002;66 (Suppl 1):S3–6. - PubMed
-
- Martin JA, Kung HC, Mathews TJ, Hoyert DL, Strobino DM, Guyer B, et al. Annual summary of vital statistics: 2006. Pediatrics. 2008;121(4):788–801. - PubMed
-
- Martin JH, BE, Sutton PD, et al. National vital statistics reports. National Center for Health Statistics; 2009. Births: Final data for 2006.
-
- Yang Q, Chen H, Correa A, Devine O, Mathews TJ, Honein MA. Racial differences in infant mortality attributable to birth defects in the United States, 1989–2002. Birth Defects Res A Clin Mol Teratol. 2006;76(10):706–713. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
