

Impact of surveillance of hospital-acquired infections on the incidence of ventilator-associated pneumonia in intensive care units: a quasi-experimental study
- PMID: 22909033
- PMCID: PMC3580751
- DOI: 10.1186/cc11484
Impact of surveillance of hospital-acquired infections on the incidence of ventilator-associated pneumonia in intensive care units: a quasi-experimental study
Abstract
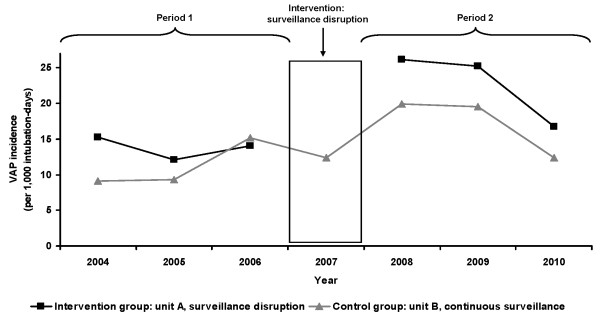
Introduction: The preventive impact of hospital-acquired infection (HAI) surveillance is difficult to assess. Our objective was to investigate the effect of HAI surveillance disruption on ventilator-associated pneumonia (VAP) incidence.
Methods: A quasi-experimental study with an intervention group and a control group was conducted between 1 January 2004 and 31 December 2010 in two intensive care units (ICUs) of a university hospital that participated in a national HAI surveillance network. Surveillance was interrupted during the year 2007 in unit A (intervention group) and was continuous in unit B (control group). Period 1 (pre-test period) comprised patients hospitalized during 2004 to 2006, and period 2 (post-test period) involved patients hospitalized during 2008 to 2010. Patients hospitalized ≥ 48 hours and intubated during their stay were included. Multivariate Poisson regression was fitted to ascertain the influence of surveillance disruption.
Results: A total of 2,771 patients, accounting for 19,848 intubation-days at risk, were studied; 307 had VAP. The VAP attack rate increased in unit A from 7.8% during period 1 to 17.1% during period 2 (P <0.001); in unit B, it was 7.2% and 11.2% for the two periods respectively (P = 0.17). Adjusted VAP incidence rose in unit A after surveillance disruption (incidence rate ratio = 2.17, 95% confidence interval 1.05 to 4.47, P = 0.036), independently of VAP trend; no change was observed in unit B. All-cause mortality and length of stay increased (P = 0.028 and P = 0.038, respectively) in unit A between periods 1 and 2. In unit B, no change in mortality was observed (P = 0.22), while length of stay decreased between periods 1 and 2 (P = 0.002).
Conclusions: VAP incidence, length of stay and all-cause mortality rose after HAI surveillance disruption in ICU, which suggests a specific effect of HAI surveillance on VAP prevention and reinforces the role of data feedback and counselling as a mechanism to facilitate performance improvement.
Figures
Comment in
-
Advancing the science of ventilator-associated pneumonia surveillance.Crit Care. 2012 Oct 31;16(5):165. doi: 10.1186/cc11656. Crit Care. 2012. PMID: 23113957 Free PMC article.
References
-
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165:867–903. - PubMed
-
- French National Health Institute: Surveillance des infections nosocomiales en réanimation adulte - Réseau REA-Raisin, France, Résultats. 2010. http://www.invs.sante.fr
-
- Bekaert M, Timsit JF, Vansteelandt S, Depuydt P, Vésin A, Garrouste-Orgeas M, Decruyenaere J, Clec'h C, Azoulay E, Benoit D. Outcomerea Study Group. Attributable mortality of ventilator-associated pneumonia: a reappraisal using causal analysis. Am J Respir Crit Care Med. 2011;184:1133–1139. doi: 10.1164/rccm.201105-0867OC. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
