

Remote ischemic perconditioning is effective alone and in combination with intravenous tissue-type plasminogen activator in murine model of embolic stroke
- PMID: 22910893
- PMCID: PMC3740528
- DOI: 10.1161/STROKEAHA.112.660373
Remote ischemic perconditioning is effective alone and in combination with intravenous tissue-type plasminogen activator in murine model of embolic stroke
Abstract
Background and purpose: Remote ischemic conditioning is cardioprotective in myocardial infarction and neuroprotective in mechanical occlusion models of stroke. However, there is no report on its therapeutic potential in a physiologically relevant embolic stroke model (embolic middle cerebral artery occlusion) in combination with intravenous tissue-type plasminogen activator (tPA).
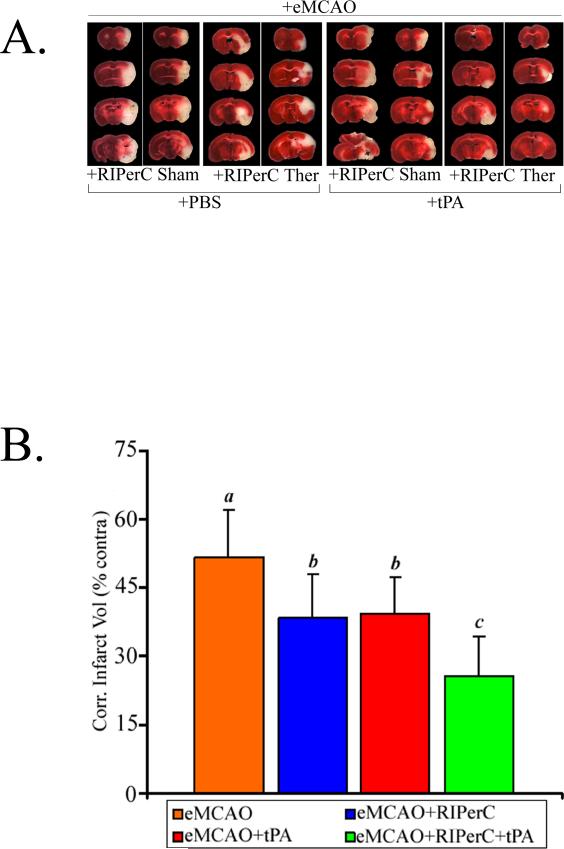
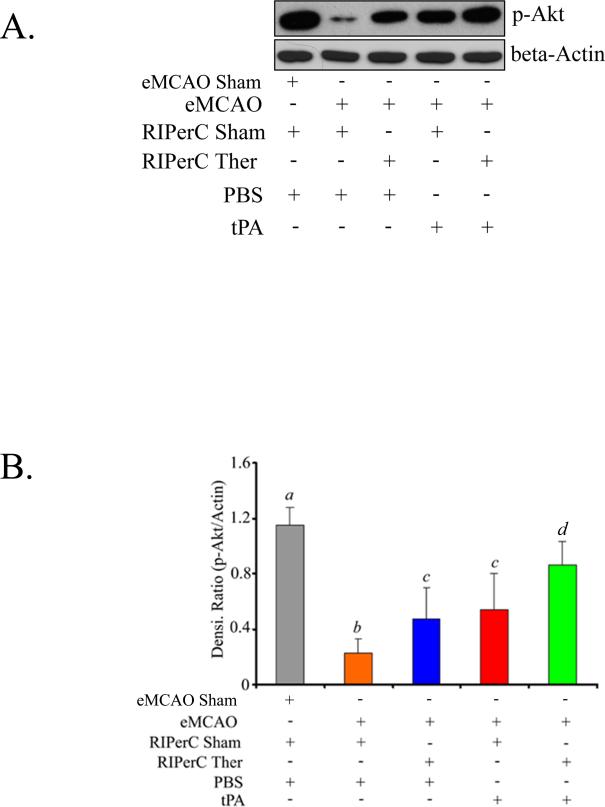
Methods: We tested remote ischemic perconditioning therapy (RIPerC) at 2 hours after embolic middle cerebral artery occlusion in the mouse with and without intravenous tPA at 4 hours. We assessed cerebral blood flow up to 6 hours, neurological deficits, injury size, and phosphorylation of Akt (Serine(473)) as a prosurvival signal in the ischemic hemisphere at 48 hours poststroke.
Results: RIPerC therapy alone improved the cerebral blood flow and neurological outcomes. tPA alone at 4 hours did not significantly improve the neurological outcome even after successful thrombolysis. Individual treatments with RIPerC and intravenous tPA reduced the infarct size (25.7% and 23.8%, respectively). Combination therapy of RIPerC and tPA resulted in additive effects in further improving the neurological outcome and reducing the infarct size (50%). All the therapeutic treatments upregulated phosphorylation of Akt in the ischemic hemisphere.
Conclusions: RIPerC is effective alone after embolic middle cerebral artery occlusion and has additive effects in combination with intravenous tPA. RIPerC may be a simple, safe, and inexpensive combination therapy with intravenous tPA.
Figures

Comment in
-
Letter by Hanss regarding article, "Remote ischemic perconditioning is effective alone and in combination with intravenous tissue-type plasminogen activator in murine model of embolic stroke".Stroke. 2013 Apr;44(4):e36. doi: 10.1161/STROKEAHA.112.679951. Stroke. 2013. PMID: 23529915 No abstract available.
-
Response to letter regarding article, "Remote ischemic perconditioning is effective alone and in combination with intravenous tissue-type".Stroke. 2013 Apr;44(4):e37. doi: 10.1161/strokeaha.111.000541. Stroke. 2013. PMID: 23646369 No abstract available.
References
-
- Albers GW, Goldstein LB, Hess DC, Wechsler LR, Furie KL, Gorelick PB, et al. Stroke treatment academic industry roundtable (stair) recommendations for maximizing the use of intravenous thrombolytics and expanding treatment options with intra-arterial and neuroprotective therapies. Stroke. 2011;42:2645–2650. - PubMed
-
- Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: A delay of lethal cell injury in ischemic myocardium. Circulation. 1986;74:1124–1136. - PubMed
-
- Vander Heide R. Clinically useful cardioprotection: Ischemic preconditioning then and now. J Cardiovasc Pharmacol Ther. 2011;16:251–254. - PubMed
-
- Przyklenk K, Whittaker P. Remote ischemic preconditioning: Current knowledge, unresolved questions, and future priorities. J Cardiovasc Pharmacol Ther. 2011;16:255–259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
