

Predictive accuracy of the Liverpool Lung Project risk model for stratifying patients for computed tomography screening for lung cancer: a case-control and cohort validation study
- PMID: 22910935
- PMCID: PMC3723683
- DOI: 10.7326/0003-4819-157-4-201208210-00004
Predictive accuracy of the Liverpool Lung Project risk model for stratifying patients for computed tomography screening for lung cancer: a case-control and cohort validation study
Abstract
Background: External validation of existing lung cancer risk prediction models is limited. Using such models in clinical practice to guide the referral of patients for computed tomography (CT) screening for lung cancer depends on external validation and evidence of predicted clinical benefit.
Objective: To evaluate the discrimination of the Liverpool Lung Project (LLP) risk model and demonstrate its predicted benefit for stratifying patients for CT screening by using data from 3 independent studies from Europe and North America.
Design: Case-control and prospective cohort study.
Setting: Europe and North America.
Patients: Participants in the European Early Lung Cancer (EUELC) and Harvard case-control studies and the LLP population-based prospective cohort (LLPC) study.
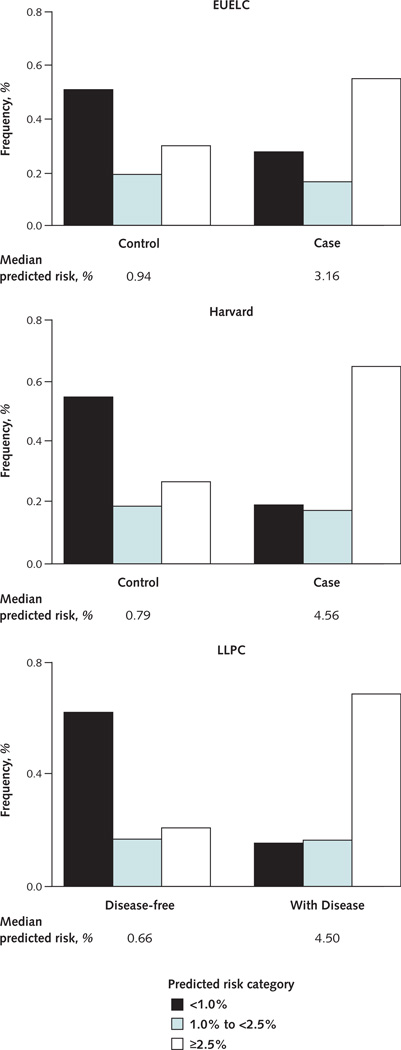
Measurements: 5-year absolute risks for lung cancer predicted by the LLP model.
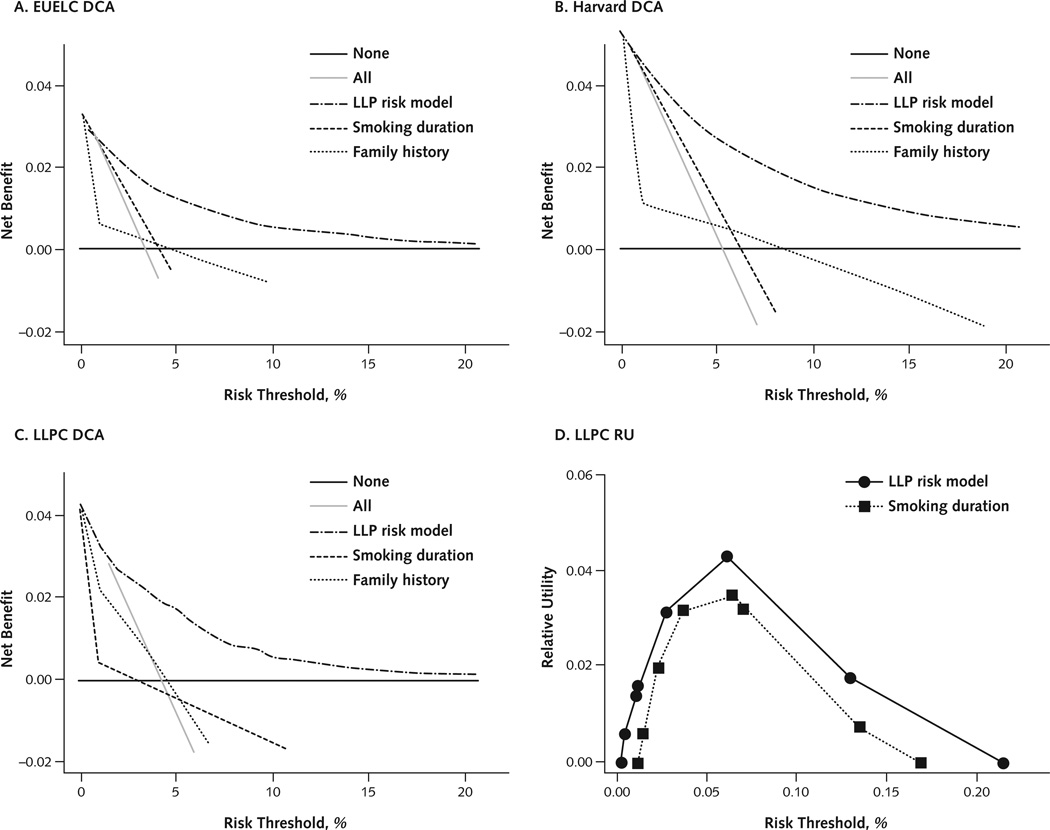
Results: The LLP risk model had good discrimination in both the Harvard (area under the receiver-operating characteristic curve [AUC], 0.76 [95% CI, 0.75 to 0.78]) and the LLPC (AUC, 0.82 [CI, 0.80 to 0.85]) studies and modest discrimination in the EUELC (AUC, 0.67 [CI, 0.64 to 0.69]) study. The decision utility analysis, which incorporates the harms and benefit of using a risk model to make clinical decisions, indicates that the LLP risk model performed better than smoking duration or family history alone in stratifying high-risk patients for lung cancer CT screening.
Limitations: The model cannot assess whether including other risk factors, such as lung function or genetic markers, would improve accuracy. Lack of information on asbestos exposure in the LLPC limited the ability to validate the complete LLP risk model.
Conclusion: Validation of the LLP risk model in 3 independent external data sets demonstrated good discrimination and evidence of predicted benefits for stratifying patients for lung cancer CT screening. Further studies are needed to prospectively evaluate model performance and evaluate the optimal population risk thresholds for initiating lung cancer screening.
Conflict of interest statement
Figures
Comment in
-
Beyond the usual prediction accuracy metrics: reporting results for clinical decision making.Ann Intern Med. 2012 Aug 21;157(4):294-5. doi: 10.7326/0003-4819-157-4-201208210-00014. Ann Intern Med. 2012. PMID: 22910942 No abstract available.
-
Predictive accuracy of the Liverpool Lung Project risk model.Ann Intern Med. 2013 Apr 2;158(7):568. doi: 10.7326/0003-4819-158-7-201304020-00014. Ann Intern Med. 2013. PMID: 23546573 No abstract available.
-
In response. Predictive accuracy of the Liverpool Lung Project risk model.Ann Intern Med. 2013 Apr 2;158(7):568-9. doi: 10.7326/0003-4819-158-7-201304020-00015. Ann Intern Med. 2013. PMID: 23546574 No abstract available.
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. [PMID: 15761078] - PubMed
-
- Schiller JH, Harrington D, Belani CP, Langer C, Sandler A, Krook J, et al. Eastern Cooperative Oncology Group. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med. 2002;346:92–98. [PMID: 11784875] - PubMed
-
- van Klaveren RJ, Habbema JDF, Pedersen JH, de Koning HJ, Oudkerk M, Hoogsteden HC. Lung cancer screening by low-dose spiral computed tomography. Eur Respir J. 2001;18:857–866. [PMID: 11757637] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases