

Antiretroviral therapy for prevention of tuberculosis in adults with HIV: a systematic review and meta-analysis
- PMID: 22911011
- PMCID: PMC3404110
- DOI: 10.1371/journal.pmed.1001270
Antiretroviral therapy for prevention of tuberculosis in adults with HIV: a systematic review and meta-analysis
Abstract
Background: Human immunodeficiency virus (HIV) infection is the strongest risk factor for developing tuberculosis and has fuelled its resurgence, especially in sub-Saharan Africa. In 2010, there were an estimated 1.1 million incident cases of tuberculosis among the 34 million people living with HIV worldwide. Antiretroviral therapy has substantial potential to prevent HIV-associated tuberculosis. We conducted a systematic review of studies that analysed the impact of antiretroviral therapy on the incidence of tuberculosis in adults with HIV infection.
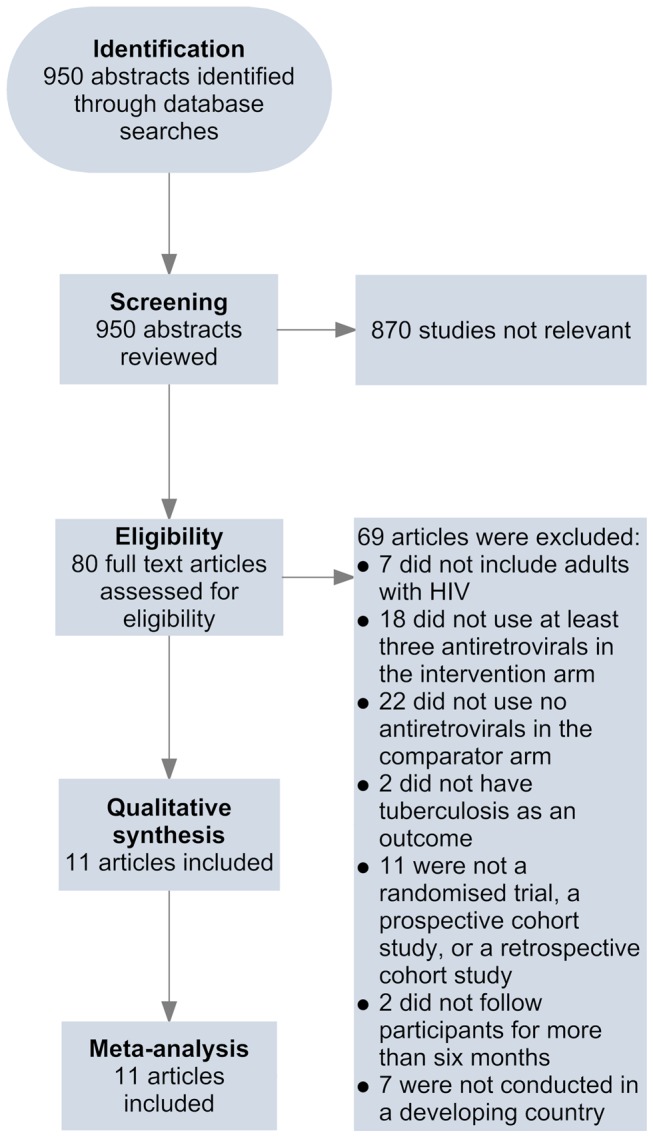
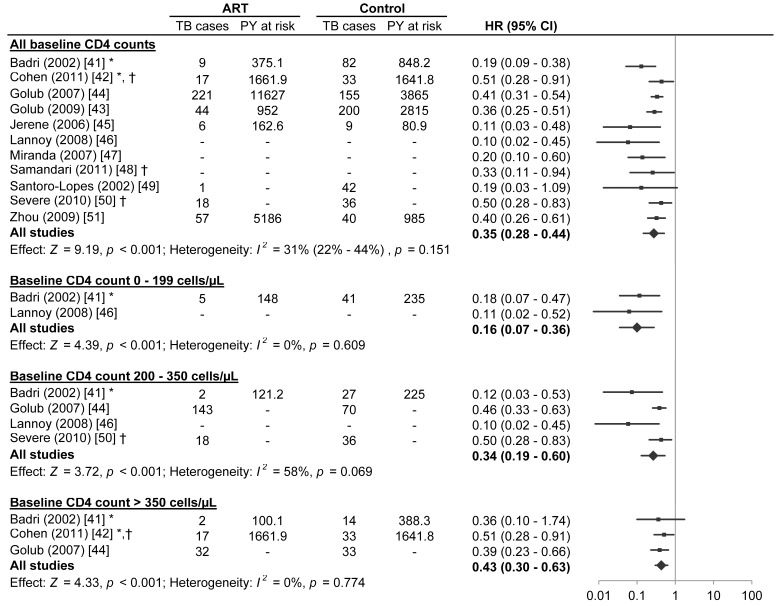
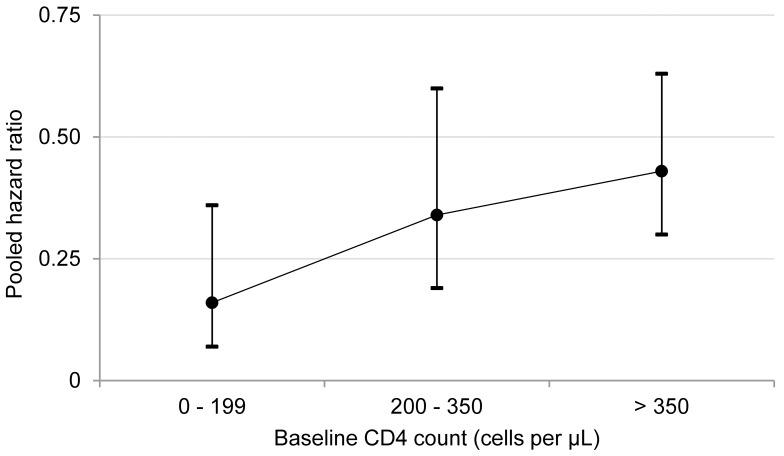
Methods and findings: PubMed, Embase, African Index Medicus, LILACS, and clinical trial registries were systematically searched. Randomised controlled trials, prospective cohort studies, and retrospective cohort studies were included if they compared tuberculosis incidence by antiretroviral therapy status in HIV-infected adults for a median of over 6 mo in developing countries. For the meta-analyses there were four categories based on CD4 counts at antiretroviral therapy initiation: (1) less than 200 cells/µl, (2) 200 to 350 cells/µl, (3) greater than 350 cells/µl, and (4) any CD4 count. Eleven studies met the inclusion criteria. Antiretroviral therapy is strongly associated with a reduction in the incidence of tuberculosis in all baseline CD4 count categories: (1) less than 200 cells/µl (hazard ratio [HR] 0.16, 95% confidence interval [CI] 0.07 to 0.36), (2) 200 to 350 cells/µl (HR 0.34, 95% CI 0.19 to 0.60), (3) greater than 350 cells/µl (HR 0.43, 95% CI 0.30 to 0.63), and (4) any CD4 count (HR 0.35, 95% CI 0.28 to 0.44). There was no evidence of hazard ratio modification with respect to baseline CD4 count category (p = 0.20).
Conclusions: Antiretroviral therapy is strongly associated with a reduction in the incidence of tuberculosis across all CD4 count strata. Earlier initiation of antiretroviral therapy may be a key component of global and national strategies to control the HIV-associated tuberculosis syndemic.
Review registration: International Prospective Register of Systematic Reviews CRD42011001209 Please see later in the article for the Editors' Summary.
Conflict of interest statement
TRS received a research grant from Bristol Myers Squibb for HIV observational studies, a research grant from Pfizer for HIV observational studies, and research grant support from the US National Institutes of Health and the US Centers for Disease Control and Prevention. TRS is also a member of a data safety monitoring board for Otsuka. ABS, HG, DS, and RMG work for WHO. The authors alone are responsible for the views expressed in this publication and they do not necessarily represent the decisions or policies of the World Health Organization. All other authors have declared that no competing interests exist.
Figures
References
-
- Harries AD, Zachariah R, Corbett EL, Lawn SD, Santos-Filho ET, et al. (2010) The HIV-associated tuberculosis epidemic—when will we act? Lancet 375: 1906–1919. - PubMed
-
- Joint United Nations Programme on HIV/AIDS (2011) World AIDS Day report 2011. Available: http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspubl.... Accessed 23 November 2011.
-
- World Health Organization (2011) Global tuberculosis control 2011. Available: http://www.who.int/entity/tb/publications/global_report/2011/gtbr11_full.... Accessed 14 October 2011.
-
- The United Nations (2011) The Millenium Development Goals report. Available: http://mdgs.un.org/unsd/mdg/Resources/Static/Products/Progress2011/11-31.... Accessed 18 July 2011.
-
- Stop TB Partnership (2010) The global plan to stop TB: 2011–2015. Available: http://www.stoptb.org/assets/documents/global/plan/TB_GlobalPlanToStopTB.... Accessed 7 February 2011.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
