

Early risk factors for enlargement of the tracheoesophageal puncture after total laryngectomy: nodal metastasis and extent of surgery
- PMID: 22911245
- PMCID: PMC4095893
- DOI: 10.1001/archoto.2012.1753
Early risk factors for enlargement of the tracheoesophageal puncture after total laryngectomy: nodal metastasis and extent of surgery
Abstract
Objective: To determine the early risk factors for enlargement of the tracheoesophageal puncture (TEP) after total laryngectomy.
Design: Retrospective cohort study.
Setting: The University of Texas MD Anderson Cancer Center, Houston.
Patients: The study included 194 patients who underwent total laryngectomy (with or without pharyngectomy) and TEP (2003-2008).
Main outcome measures: Multiple logistic regression methods were used to evaluate early risk factors for an enlarged TEP.
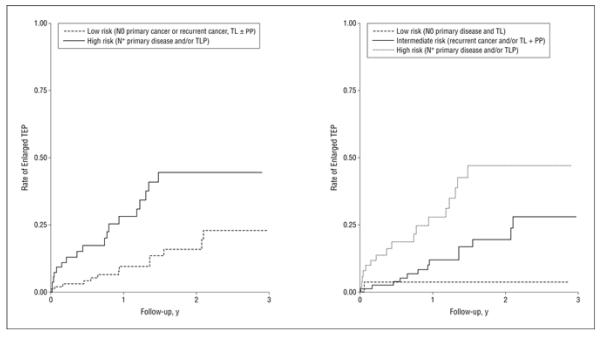
Results: The incidence of an enlarged TEP was 18.6% (36 of 194 patients). After adjustment for follow-up time and radiotherapy history, patients with nodal metastases had a significantly higher risk of TEP enlargement (adjusted odds ratio, 6.6; 95% CI, 1.6-26.6) than those with node-negative disease. Total laryngopharyngectomy significantly increased the risk of an enlarged TEP (adjusted odds ratio, 4.5; 95% CI, 1.4-14.7) compared with simple total laryngectomy. Before multivariable adjustment, the preoperative body mass index was also significantly associated with enlargement (P for trend, .04).
Conclusions: These data suggest that 2 clinical factors-nodal staging and extent of resection-may help identify those at highest risk for TEP enlargement early after surgery. These simple indicators may ultimately aid in patient selection and prevention of an enlarged TEP after total laryngectomy.
Figures
References
-
- Xi S. Effectiveness of voice rehabilitation on vocalisation in postlaryngectomy patients: a systematic review. Int J Evid Based Healthc. 2010;8(4):256–258. - PubMed
-
- Op de Coul BM, Hilgers FJ, Balm AJ, Tan IB, van den Hoogen FJ, van Tinteren H. A decade of postlaryngectomy vocal rehabilitation in 318 patients: a single Institution’s experience with consistent application of provox indwelling voice prostheses. Arch Otolaryngol Head Neck Surg. 2000;126(11):1320–1328. - PubMed
