

Hepatitis B and C co-infection are independent predictors of progressive kidney disease in HIV-positive, antiretroviral-treated adults
- PMID: 22911697
- PMCID: PMC3401192
- DOI: 10.1371/journal.pone.0040245
Hepatitis B and C co-infection are independent predictors of progressive kidney disease in HIV-positive, antiretroviral-treated adults
Abstract
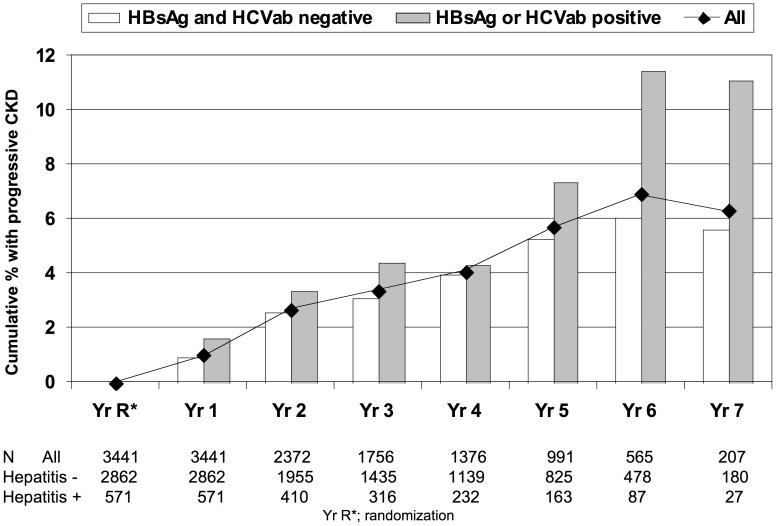
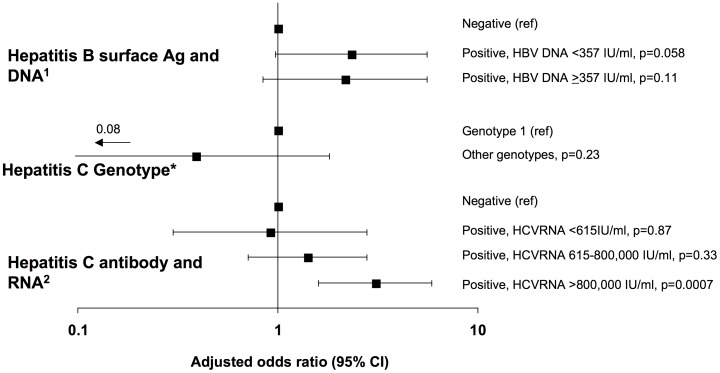
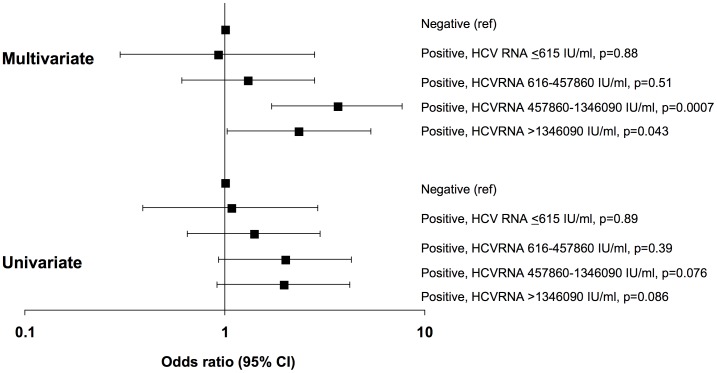
Chronic kidney disease (CKD) is an important cause of morbidity and mortality in HIV-positive individuals. Hepatitis C (HCV) co-infection has been associated with increased risk of CKD, but prior studies lack information on potential mechanisms. We evaluated the association between HCV or hepatitis B (HBV) co-infection and progressive CKD among 3,441 antiretroviral-treated clinical trial participants. Progressive CKD was defined as the composite of end-stage renal disease, renal death, or significant glomerular filtration rate (eGFR) decline (25% decline to eGFR <60 mL/min/1.73 m(2) or 25% decline with a baseline <60). Generalized Estimating Equations were used to model the odds of progressive CKD. At baseline, 13.8% and 3.3% of participants were co-infected with HCV and HBV, respectively. Median eGFR was 111, and 3.7% developed progressive CKD. After adjustment, the odds of progressive CKD were increased in participants with HCV (OR 1.72, 95% CI 1.07-2.76) or HBV (OR 2.26, 95% CI 1.15-4.44). Participants with undetectable or low HCV-RNA had similar odds of progressive CKD as HCV seronegative participants, while participants with HCV-RNA >800,000 IU/ml had increased odds (OR 3.07; 95% CI 1.60-5.90). Interleukin-6, hyaluronic acid, and the FIB-4 hepatic fibrosis index were higher among participants who developed progressive CKD, but were no longer associated with progressive CKD after adjustment. Future studies should validate the relationship between HCV viremia and CKD.
Trial registration: ClinicalTrials.gov NCT00027352; NCT00004978.
Conflict of interest statement
Figures
References
-
- El-Sadr WM, Lundgren JD, Neaton JD, Gordin F, Abrams D, et al. CD4+ count-guided interruption of antiretroviral treatment. N Engl J Med. 2006;355:2283–2296. - PubMed
-
- Gupta SK, Eustace JA, Winston JA, Boydstun II, Ahuja TS, et al. Guidelines for the management of chronic kidney disease in HIV-infected patients: recommendations of the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2005;40:1559–1585. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
