

Poverty increases type 2 diabetes incidence and inequality of care despite universal health coverage
- PMID: 22912425
- PMCID: PMC3476930
- DOI: 10.2337/dc11-2052
Poverty increases type 2 diabetes incidence and inequality of care despite universal health coverage
Abstract
Objective: The discrepancy of diabetes incidence and care between socioeconomic statuses has seldom been studied concurrently in nations with universal health coverage. We aimed to delineate whether income disparity is associated with diabetes incidence and inequality of care under a national health insurance (NHI) program in Asia.
Research design and methods: From the Taiwan NHI database in 2000, a representative cohort aged ≥20 years and free of diabetes (n = 600,662) were followed up until 2005. We regarded individuals exempt from paying the NHI premium as being poor. Adjusted hazard ratios (HRs) were used to discover any excess risk of diabetes in the poor population. The indicators used to evaluate quality of diabetes care included the proportion of diabetic patients identified through hospitalization, visits to diabetes clinics, and completion of recommended diabetes tests.
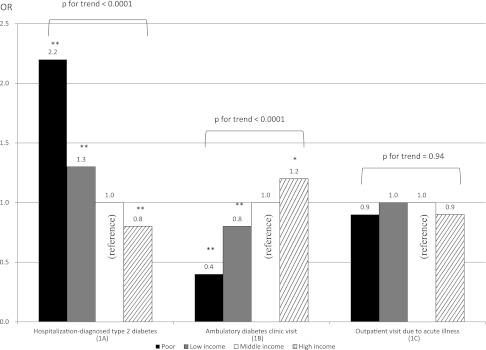
Results: The incidence of type 2 diabetes in the poor population was 20.4 per 1,000 person-years (HR, 1.5; 95% CI, 1.3-1.7). Compared with their middle-income counterparts, the adjusted odds ratio (OR) for the poor population incidentally identified as having diabetes through hospitalization was 2.2 (P < 0.001). Poor persons with diabetes were less likely to visit any diabetes clinic (OR, 0.4; P < 0.001). The ORs for the poor population with diabetes to receive tests for glycated hemoglobin, low-density lipoprotein cholesterol, triglycerides, and retinopathy were 0.6 (0.4-0.9), 0.4 (0.2-0.7), 0.5 (0.4-0.8), and 0.4 (0.2-0.9), respectively.
Conclusions: Poverty is associated not only with higher diabetes incidence but also with inequality of diabetes care in a northeast Asian population, despite universal health coverage.
Figures
References
-
- Robbins JM, Vaccarino V, Zhang H, Kasl SV. Socioeconomic status and diagnosed diabetes incidence. Diabetes Res Clin Pract 2005;68:230–236 - PubMed
-
- Everson SA, Maty SC, Lynch JW, Kaplan GA. Epidemiologic evidence for the relation between socioeconomic status and depression, obesity, and diabetes. J Psychosom Res 2002;53:891–895 - PubMed
-
- Rathmann W, Strassburger K, Heier M, et al. Incidence of Type 2 diabetes in the elderly German population and the effect of clinical and lifestyle risk factors: KORA S4/F4 cohort study. Diabet Med 2009;26:1212–1219 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
