

Medication nonadherence in diabetes: longitudinal effects on costs and potential cost savings from improvement
- PMID: 22912429
- PMCID: PMC3507586
- DOI: 10.2337/dc12-0572
Medication nonadherence in diabetes: longitudinal effects on costs and potential cost savings from improvement
Abstract
Objective: To examine the longitudinal effects of medication nonadherence (MNA) on key costs and estimate potential savings from increased adherence using a novel methodology that accounts for shared correlation among cost categories.
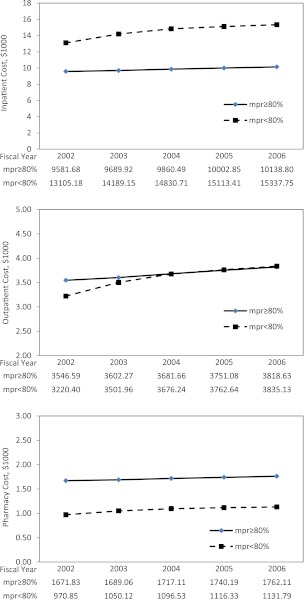
Research design and methods: Veterans with type 2 diabetes (740,195) were followed from January 2002 until death, loss to follow-up, or December 2006. A novel multivariate, generalized, linear, mixed modeling approach was used to assess the differential effect of MNA, defined as medication possession ratio (MPR) ≥0.8 on healthcare costs. A sensitivity analysis was performed to assess potential cost savings at different MNA levels using the Consumer Price Index to adjust estimates to 2012 dollar value.
Results: Mean MPR for the full sample over 5 years was 0.78, with a mean of 0.93 for the adherent group and 0.58 for the MNA group. In fully adjusted models, all annual cost categories increased ∼3% per year (P = 0.001) during the 5-year study time period. MNA was associated with a 37% lower pharmacy cost, 7% lower outpatient cost, and 41% higher inpatient cost. Based on sensitivity analyses, improving adherence in the MNA group would result in annual estimated cost savings ranging from ∼$661 million (MPR <0.6 vs. ≥0.6) to ∼$1.16 billion (MPR <1 vs. 1). Maximal incremental annual savings would occur by raising MPR from <0.8 to ≥0.8 ($204,530,778) among MNA subjects.
Conclusions: Aggressive strategies and policies are needed to achieve optimal medication adherence in diabetes. Such approaches may further the so-called "triple aim" of achieving better health, better quality care, and lower cost.
Figures
References
-
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: General Information and Estimates on Diabetes in the United States Atlanta, GA, U.S. Department of Health and Human Services, 2011. Available from http://www.cdc.gov/diabetes/pubs/factsheet11.htm
-
- Narayan KM, Boyle JP, Geiss LS, Saaddine JB, Thompson TJ. Impact of recent increase in incidence on future diabetes burden: U.S., 2005-2050. Diabetes Care 2006;29:2114–2116 - PubMed
-
- Agency for Healthcare Quality and Research. 2010 National Health Disparities Report Rockville, MD, U.S. Department of Health and Human Services, 2010 (Rep. no. 11-0005). Available from http://www.cbo.gov/publication/41656
-
- Nathan DM, Buse JB, Davidson MB, et al. American Diabetes Association. European Association for Study of Diabetes Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009;32:193–203 - PMC - PubMed
-
- U.S. Department of Veterans Affairs. VA/DoD clinical practice guidleline for the management of diabetes [Internet], 2011. Available from http://www.healthquality.va.gov/diabetes/DM2010_FUL-v4e.pdf Accessed 6 December 2011
