

Comparative study of esophageal stent and feeding gastrostomy/jejunostomy for tracheoesophageal fistula caused by esophageal squamous cell carcinoma
- PMID: 22912737
- PMCID: PMC3418295
- DOI: 10.1371/journal.pone.0042766
Comparative study of esophageal stent and feeding gastrostomy/jejunostomy for tracheoesophageal fistula caused by esophageal squamous cell carcinoma
Abstract
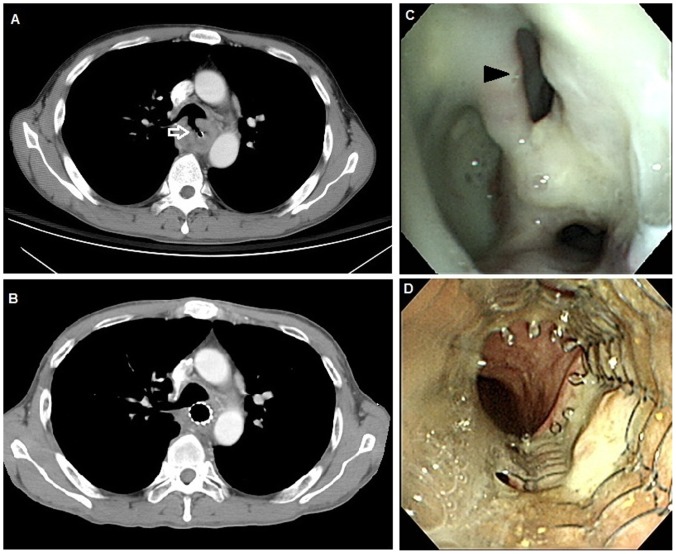
Background: A malignant tracheoesophageal/bronchoesophageal fistula (TEF) is a life-threatening complication of esophageal squamous cell carcinoma. A feeding gastrostomy/jejunostomy had been the most common treatment method for patients with TEF before the era of stenting. The aim of this retrospective study is to compare the prognosis of esophageal squamous cell carcinoma patients with TEF treated with an esophageal metallic stent to those treated with a feeding gastrostomy/jejunostomy.
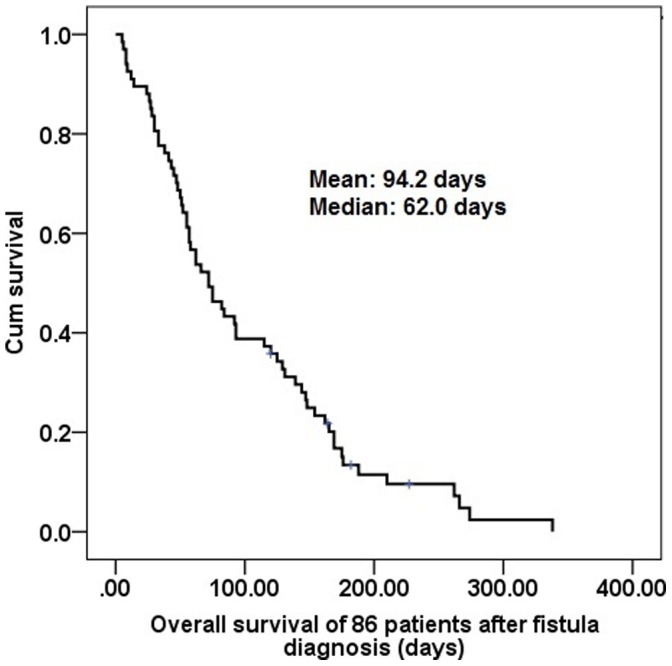
Methods: We retrospectively reviewed a total of 1011 patients with esophageal squamous cell carcinoma between 1996 and 2011 at Kaohsiung Chang Gung Memorial Hospital, and 86 patients with TEF (8.5%) were identified. The overall survival and other clinical data were compared between 30 patients treated with an esophageal metallic stent and 35 patients treated with a feeding gastrostomy/jejunostomy.
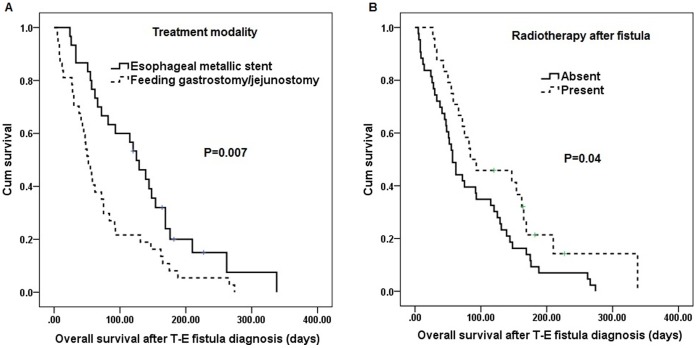
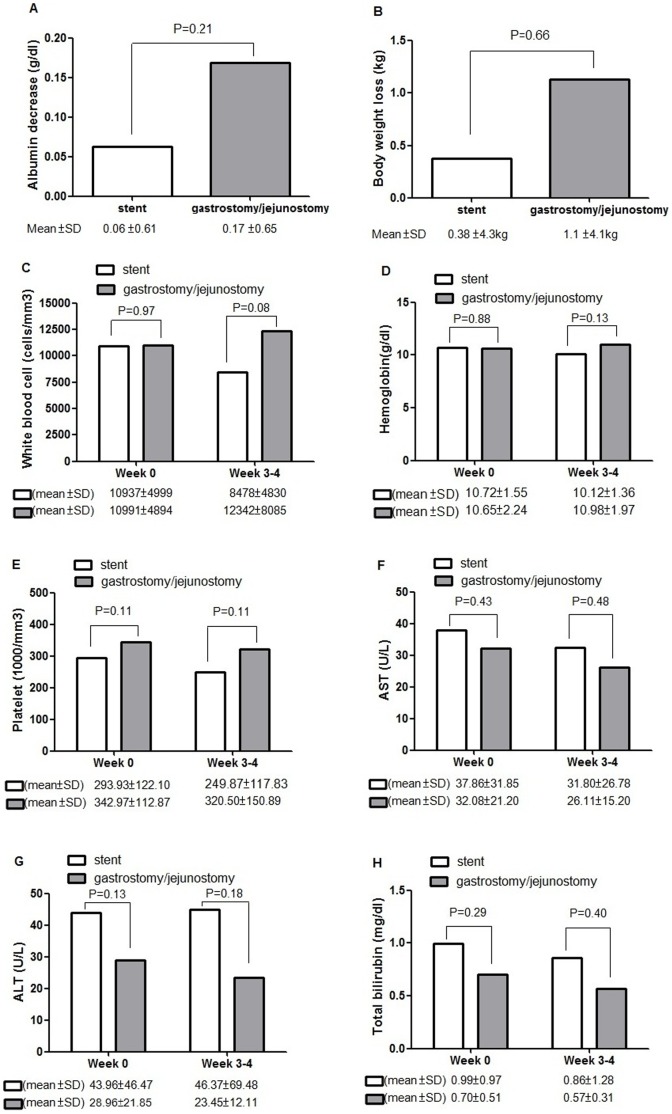
Results: Among the 65 patients receiving either an esophageal metallic stent or a feeding gastrostomy/jejunostomy, univariate analysis showed that treatment modality with an esophageal metallic stent (P = 0.007) and radiotherapy treatment after fistula diagnosis (P = 0.04) were predictive of superior overall survival. In the multivariate comparison, treatment modality with an esophageal metallic stent (P = 0.026, odds ratio: 1.859) represented the independent predictive factor of superior overall survival. There were no significant differences between groups in mean decrease in serum albumin or mean body weight loss. Compared to the feeding gastrostomy/jejunostomy group, a significantly higher proportion of patients in the stenting group (53% versus 14%, P = 0.001) were able to receive chemotherapy within 30 days after fistula diagnosis, indicating better infection control in the stenting group.
Conclusions: Compared with a feeding gastrostomy/jejunostomy, an esophageal metallic stent significantly improves overall survival in patients with malignant TEF in our retrospective analysis. Esophageal metallic stent placement may be considered the first-line of treatment for patients with malignant TEF.
Conflict of interest statement
Figures
Similar articles
-
Tracheoesophageal fistula.Chest Surg Clin N Am. 2003 May;13(2):271-89. doi: 10.1016/s1052-3359(03)00030-9. Chest Surg Clin N Am. 2003. PMID: 12755313 Review.
-
Comparative study of different treatments for malignant tracheoesophageal/bronchoesophageal fistulae.Dis Esophagus. 2009;22(6):526-31. doi: 10.1111/j.1442-2050.2009.00950.x. Epub 2009 Mar 6. Dis Esophagus. 2009. PMID: 19302211 Clinical Trial.
-
Morbidity and mortality after self-expandable metallic stent placement in patients with progressive or recurrent esophageal cancer after chemoradiotherapy.Gastrointest Endosc. 2003 Jun;57(7):882-5. doi: 10.1016/s0016-5107(03)70024-8. Gastrointest Endosc. 2003. PMID: 12776036
-
Airway Covered Metallic Stent Based on Different Fistula Location and Size in Malignant Tracheoesophageal Fistula.Am J Med Sci. 2015 Nov;350(5):364-8. doi: 10.1097/MAJ.0000000000000565. Am J Med Sci. 2015. PMID: 26422803
-
Malignant respiratory-digestive fistulas.Curr Opin Pulm Med. 2010 Jul;16(4):329-33. doi: 10.1097/MCP.0b013e3283390de8. Curr Opin Pulm Med. 2010. PMID: 20531081 Review.
Cited by
-
A novel surgical method for acquired non-malignant complicated tracheoesophageal and bronchial-gastric stump fistula: the "double patch" technique.J Thorac Dis. 2016 Nov;8(11):3225-3231. doi: 10.21037/jtd.2016.11.80. J Thorac Dis. 2016. PMID: 28066602 Free PMC article.
-
Fistulas between the Esophagus and Adjacent Vital Organs in Esophageal Cancer.Korean J Thorac Cardiovasc Surg. 2020 Aug 5;53(4):211-216. doi: 10.5090/kjtcs.2020.53.4.211. Korean J Thorac Cardiovasc Surg. 2020. PMID: 32793454 Free PMC article.
-
Hsa_circ_0006948 enhances cancer progression and epithelial-mesenchymal transition through the miR-490-3p/HMGA2 axis in esophageal squamous cell carcinoma.Aging (Albany NY). 2019 Dec 26;11(24):11937-11954. doi: 10.18632/aging.102519. Epub 2019 Dec 26. Aging (Albany NY). 2019. PMID: 31881015 Free PMC article.
-
Safety and efficacy of airway stenting in patients with malignant oesophago-airway fistula.J Thorac Dis. 2018 May;10(5):2731-2739. doi: 10.21037/jtd.2018.05.19. J Thorac Dis. 2018. PMID: 29997935 Free PMC article.
-
Are single or dual luminal covered expandable metallic stents suitable for esophageal squamous cell carcinoma with esophago-airway fistula?Surg Endosc. 2017 Mar;31(3):1148-1155. doi: 10.1007/s00464-016-5084-6. Epub 2016 Jul 13. Surg Endosc. 2017. PMID: 27412126
References
-
- Balazs A, Kupcsulik PK, Galambos Z (2008) Esophagorespiratory fistulas of tumorous origin. Non-operative management of 264 cases in a 20-year period. Eur J Cardiothorac Surg 34: 1103–1107. - PubMed
-
- Martini N, Goodner JT, D’Angio GJ, Beattie EJ Jr (1970) Tracheoesophageal fistula due to cancer. J Thorac Cardiovasc Surg 59: 319–324. - PubMed
-
- Morgan RA, Ellul JP, Denton ER, Glynos M, Mason RC, et al. (1997) Malignant esophageal fistulas and perforations: management with plastic-covered metallic endoprostheses. Radiology 204: 527–532. - PubMed
-
- Gudovsky LM, Koroleva NS, Biryukov YB, Chernousov AF, Perelman MI (1993) Tracheoesophageal fistulas. Ann Thorac Surg 55: 868–875. - PubMed
-
- Hu Y, Zhao YF, Chen LQ, Zhu ZJ, Liu LX, et al. (2009) Comparative study of different treatments for malignant tracheoesophageal/bronchoesophageal fistulae. Dis Esophagus 22: 526–531. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
