

Anterior cervical discectomy with arthroplasty versus arthrodesis for single-level cervical spondylosis: a systematic review and meta-analysis
- PMID: 22912869
- PMCID: PMC3422251
- DOI: 10.1371/journal.pone.0043407
Anterior cervical discectomy with arthroplasty versus arthrodesis for single-level cervical spondylosis: a systematic review and meta-analysis
Abstract
Objective: To estimate the effectiveness of anterior cervical discectomy with arthroplasty (ACDA) compared to anterior cervical discectomy with fusion (ACDF) for patient-important outcomes for single-level cervical spondylosis.
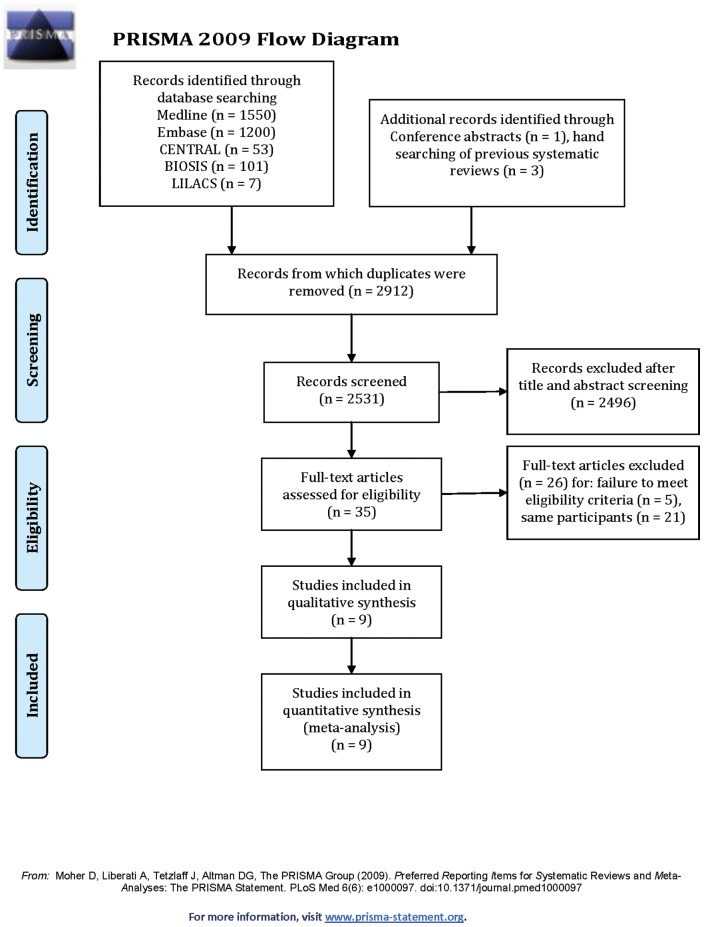
Data sources: Electronic databases (MEDLINE, EMBASE, Cochrane Register for Randomized Controlled Trials, BIOSIS and LILACS), archives of spine meetings and bibliographies of relevant articles.
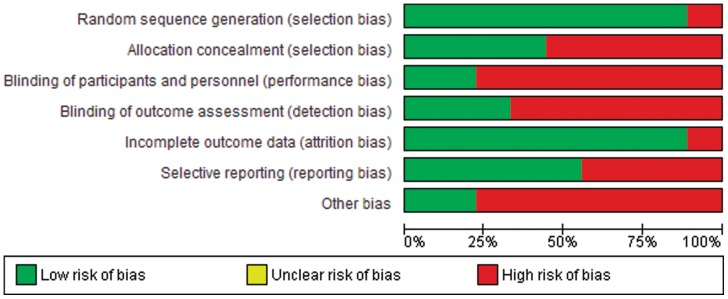
Study selection: We included RCTs of ACDF versus ACDA in adult patients with single-level cervical spondylosis reporting at least one of the following outcomes: functionality, neurological success, neck pain, arm pain, quality of life, surgery for adjacent level degeneration (ALD), reoperation and dysphonia/dysphagia. We used no language restrictions. We performed title and abstract screening and full text screening independently and in duplicate.
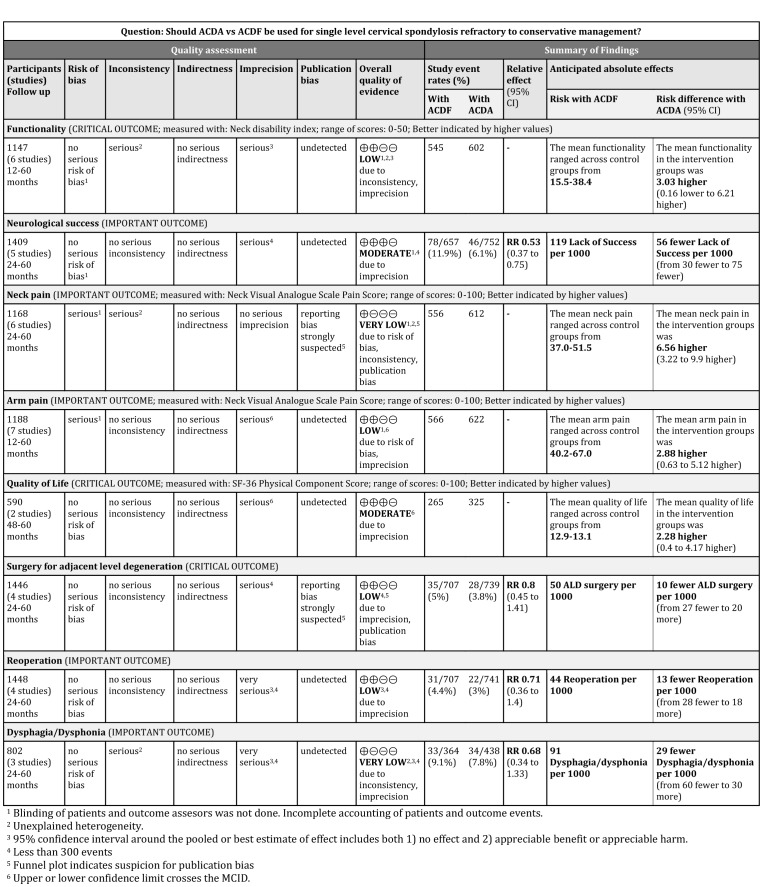
Data synthesis: We used random-effects model to pool data using mean difference (MD) for continuous outcomes and relative risk (RR) for dichotomous outcomes. We used GRADE to evaluate the quality of evidence for each outcome.
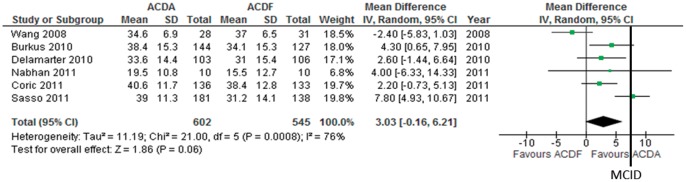
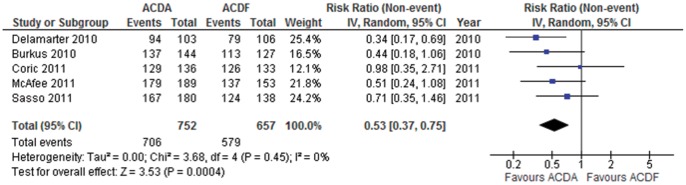
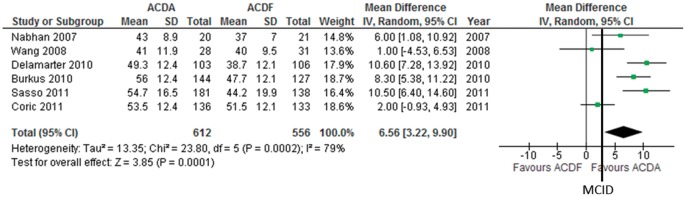
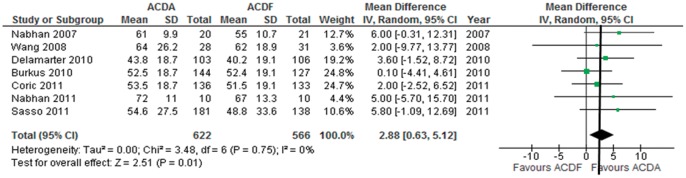
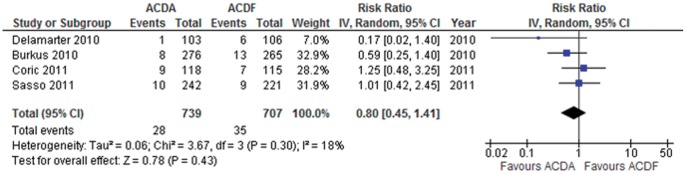
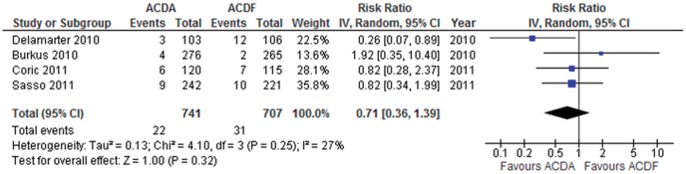
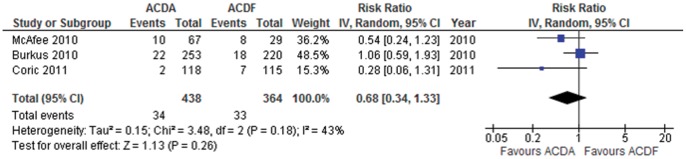
Results: Of 2804 citations, 9 articles reporting on 9 trials (1778 participants) were eligible. ACDA is associated with a clinically significant lower incidence of neurologic failure (RR = 0.53, 95% CI = 0.37-0.75, p = 0.0004) and improvement in the Neck pain visual analogue scale (VAS) (MD = 6.56, 95% CI = 3.22-9.90, p = 0.0001; Minimal clinically important difference (MCID) = 2.5. ACDA is associated with a statistically but not clinically significant improvement in Arm pain VAS and SF-36 physical component summary. ACDA is associated with non-statistically significant higher improvement in the Neck Disability Index Score and lower incidence of ALD requiring surgery, reoperation, and dysphagia/dysphonia.
Conclusions: There is no strong evidence to support the routine use of ACDA over ACDF in single-level cervical spondylosis. Current trials lack long-term data required to assess safety as well as surgery for ALD. We suggest that ACDA in patients with single level cervical spondylosis is an option although its benefits and indication over ACDF remain in question.
Conflict of interest statement
Figures

Similar articles
-
Arthroplasty versus fusion in single-level cervical degenerative disc disease.Cochrane Database Syst Rev. 2012 Sep 12;(9):CD009173. doi: 10.1002/14651858.CD009173.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2015 May 21;(5):CD009173. doi: 10.1002/14651858.CD009173.pub3. PMID: 22972137 Updated.
-
Comparison of outcomes between cervical disc arthroplasty and anterior cervical discectomy and fusion for the treatment of cervical spondylotic myelopathy: a systematic review and meta-analysis.J Neurosurg Spine. 2025 Apr 4;42(6):705-717. doi: 10.3171/2024.12.SPINE24623. Print 2025 Jun 1. J Neurosurg Spine. 2025. PMID: 40184678
-
Is anterior cervical discectomy and fusion superior to corpectomy and fusion for treatment of multilevel cervical spondylotic myelopathy? A systemic review and meta-analysis.PLoS One. 2014 Jan 28;9(1):e87191. doi: 10.1371/journal.pone.0087191. eCollection 2014. PLoS One. 2014. PMID: 24489868 Free PMC article.
-
Mid- to Long-Term Outcomes of Cervical Disc Arthroplasty versus Anterior Cervical Discectomy and Fusion for Treatment of Symptomatic Cervical Disc Disease: A Systematic Review and Meta-Analysis of Eight Prospective Randomized Controlled Trials.PLoS One. 2016 Feb 12;11(2):e0149312. doi: 10.1371/journal.pone.0149312. eCollection 2016. PLoS One. 2016. PMID: 26872258 Free PMC article.
-
Kinematics of the cervical adjacent segments after disc arthroplasty compared with anterior discectomy and fusion: a systematic review and meta-analysis.Spine (Phila Pa 1976). 2012 Oct 15;37(22 Suppl):S85-95. doi: 10.1097/BRS.0b013e31826d6628. Spine (Phila Pa 1976). 2012. PMID: 22885834
Cited by
-
Hybrid Surgery Versus Anterior Cervical Discectomy and Fusion in Multilevel Cervical Disc Diseases: A Meta-Analysis.Medicine (Baltimore). 2016 May;95(21):e3621. doi: 10.1097/MD.0000000000003621. Medicine (Baltimore). 2016. Retraction in: Medicine (Baltimore). 2019 Oct;98(40):e17483. doi: 10.1097/MD.0000000000017483. Corrected and republished in: Medicine (Baltimore). 2020 Jan;99(5):e19055. doi: 10.1097/MD.0000000000019055. PMID: 27227922 Free PMC article. Retracted. Corrected and republished. Review.
-
Cervical disc arthroplasty (CDA) versus anterior cervical discectomy and fusion (ACDF) in symptomatic cervical degenerative disc diseases (CDDDs): an updated meta-analysis of prospective randomized controlled trials (RCTs).Springerplus. 2016 Jul 27;5(1):1188. doi: 10.1186/s40064-016-2851-8. eCollection 2016. Springerplus. 2016. PMID: 27516926 Free PMC article. Review.
-
Anterior cervical discectomy and fusion versus hybrid surgery in multilevel cervical spondylotic myelopathy: A meta-analysis.Medicine (Baltimore). 2018 Aug;97(34):e11973. doi: 10.1097/MD.0000000000011973. Medicine (Baltimore). 2018. PMID: 30142827 Free PMC article. Review.
-
Magnetic resonance imaging evaluation after implantation of a titanium cervical disc prosthesis: a comparison of 1.5 and 3 Tesla magnet strength.Eur Spine J. 2013 Oct;22(10):2296-302. doi: 10.1007/s00586-013-2994-z. Epub 2013 Sep 6. Eur Spine J. 2013. PMID: 24061966 Free PMC article. Clinical Trial.
-
PEEK cages versus PMMA spacers in anterior cervical discectomy: comparison of fusion, subsidence, sagittal alignment, and clinical outcome with a minimum 1-year follow-up.ScientificWorldJournal. 2014;2014:398396. doi: 10.1155/2014/398396. Epub 2014 Jul 2. ScientificWorldJournal. 2014. PMID: 25110734 Free PMC article.
References
-
- Carette S, Fehlings MG (2005) Clinical practice. Cervical radiculopathy. N Engl J Med 353: 392–399. - PubMed
-
- Reitman CA, Hipp JA, Nguyen L, Esses SI (2004) Changes in segmental intervertebral motion adjacent to cervical arthrodesis: a prospective study. Spine (Phila Pa 1976) 29: E221–226. - PubMed
-
- Bartels RH, Donk R, Verbeek AL (2010) No justification for cervical disk prostheses in clinical practice: a meta-analysis of randomized controlled trials. Neurosurgery 66: 1153–1160; discussion 1160. - PubMed
-
- Sasso RC, Anderson PA, Riew KD, Heller JG (2011) Results of cervical arthroplasty compared with anterior discectomy and fusion: four-year clinical outcomes in a prospective, randomized controlled trial. J Bone Joint Surg Am 93: 1684–1692. - PubMed
