

Coronary microvascular dysfunction in the clinical setting: from mystery to reality
- PMID: 22915165
- PMCID: PMC3498003
- DOI: 10.1093/eurheartj/ehs246
Coronary microvascular dysfunction in the clinical setting: from mystery to reality
Abstract
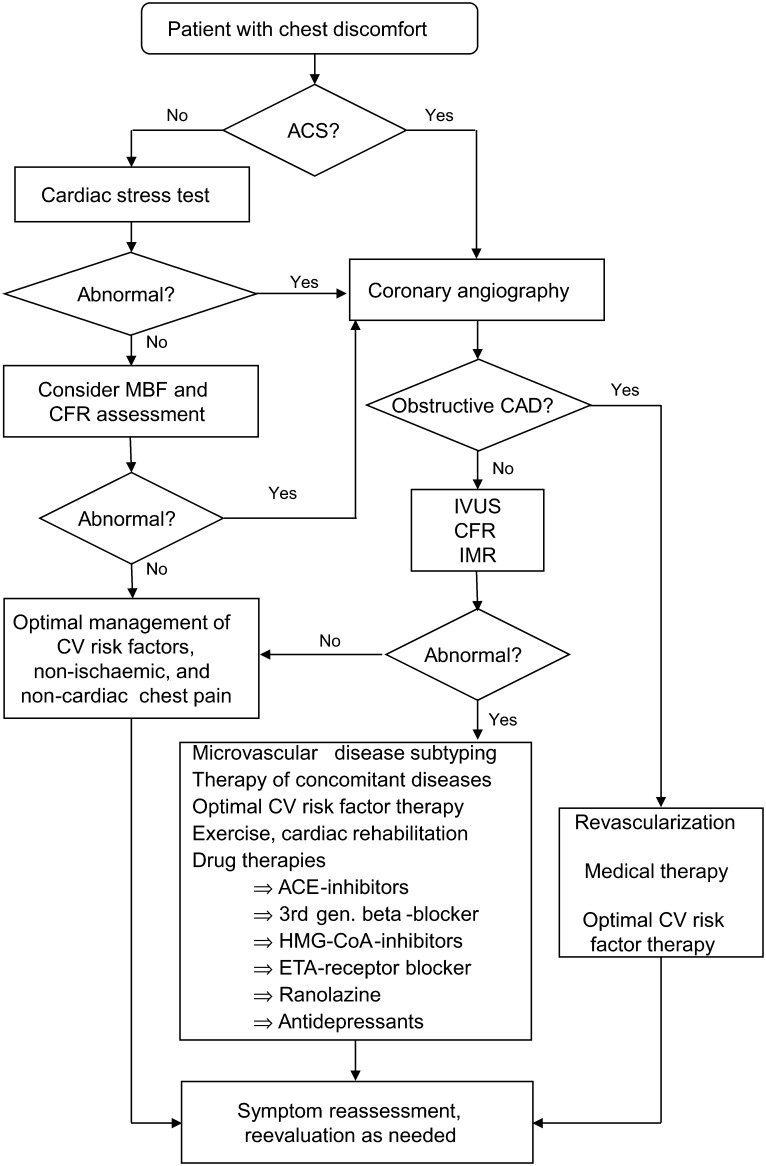
Far more extensive than the epicardial coronary vasculature that can be visualized angiographically is the coronary microcirculation, which foregoes routine imaging. Probably due to the lack of techniques able to provide tangible evidence of its crucial role, the clinical importance of coronary microvascular dysfunction is not fully appreciated. However, evidence gathered over the last several decades indicates that both functional and structural abnormalities of the coronary microvasculature can lead to myocardial ischaemia, often comparable with that caused by obstructive coronary artery disease. Indeed, a marked increase in coronary microvascular resistance can impair coronary blood flow and trigger angina pectoris, ischaemic ECG shifts, and myocardial perfusion defects, and lead to left ventricular dysfunction in patients who otherwise have patent epicardial coronary arteries. This condition--often referred to as 'chest pain with normal coronary arteries' or 'cardiac syndrome X'--encompasses several pathogenic mechanisms involving the coronary microcirculation. Of importance, coronary microvascular dysfunction can occur in conjunction with several other cardiac disease processes. In this article, we review the pathogenic mechanisms leading to coronary microvascular dysfunction and its diagnostic assessment, as well as the different clinical presentations and prognostic implications of microvascular angina. As such, this review aims to remove at least some of the mystery surrounding the notion of coronary microvascular dysfunction and to show why it represents a true clinical entity.
Figures
References
-
- Kemp HG, Jr, Vokonas PS, Cohn PF, Gorlin R. The anginal syndrome associated with normal coronary arteriograms. Report of a six year experience. Am J Med. 1973;54:735–742. doi:10.1016/0002-9343(73)90060-0. - DOI - PubMed
-
- Kaski JC. Pathophysiology and management of patients with chest pain and normal coronary arteriograms (cardiac syndrome X) Circulation. 2004;109:568–572. doi:10.1161/01.CIR.0000116601.58103.62. - DOI - PubMed
-
- Patel B, Fisher M. Therapeutic advances in myocardial microvascular resistance: unravelling the enigma. Pharmacol Ther. 2010;127:131–147. doi:10.1016/j.pharmthera.2010.04.014. - DOI - PubMed
-
- Camici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med. 2007;356:830–840. doi:10.1056/NEJMra061889. - DOI - PubMed
-
- Kuo L, Chilian WM, Davis MJ. Coronary arteriolar myogenic response is independent of endothelium. Circ Res. 1990;66:860–866. doi:10.1161/01.RES.66.3.860. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
