

Objective assessment in residency-based training for transoral robotic surgery
- PMID: 22915265
- PMCID: PMC4572744
- DOI: 10.1002/lary.23369
Objective assessment in residency-based training for transoral robotic surgery
Abstract
Objectives/hypothesis: To develop a robotic surgery training regimen integrating objective skill assessment for otolaryngology and head and neck surgery trainees consisting of training modules of increasing complexity leading up to procedure-specific training. In particular, we investigated applications of such a training approach for surgical extirpation of oropharyngeal tumors via a transoral approach using the da Vinci robotic system.
Study design: Prospective blinded data collection and objective evaluation (Objective Structured Assessment of Technical Skills [OSATS]) of three distinct phases using the da Vinci robotic surgical system in an academic university medical engineering/computer science laboratory setting.
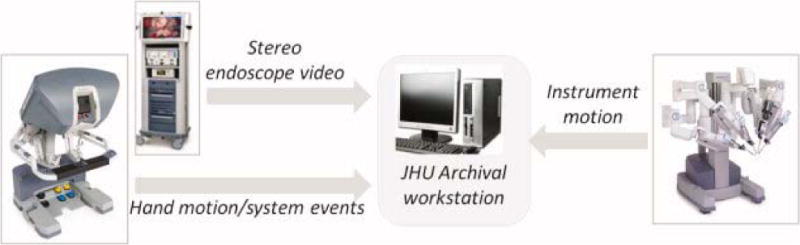
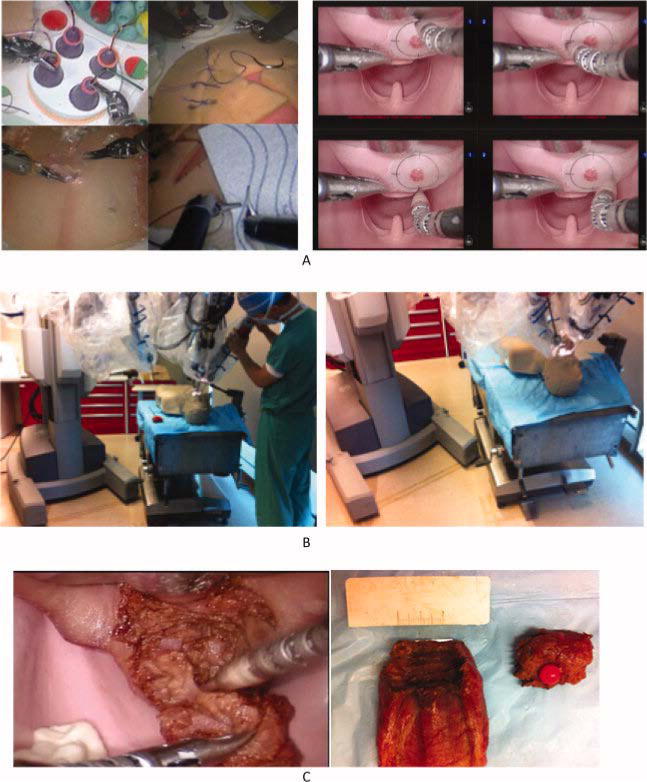
Methods: Between September 2010 and July 2011, eight otolaryngology-head and neck surgery residents and four staff experts from an academic hospital participated in three distinct phases of robotic surgery training involving 1) robotic platform operational skills, 2) set up of the patient side system, and 3) a complete ex vivo surgical extirpation of an oropharyngeal tumor located in the base of tongue. Trainees performed multiple (four) approximately equally spaced training sessions in each stage of the training. In addition to trainees, baseline performance data were obtained for the experts. Each surgical stage was documented with motion and event data captured from the application programming interfaces of the da Vinci system, as well as separate video cameras as appropriate. All data were assessed using automated skill measures of task efficiency and correlated with structured assessment (OSATS and similar Likert scale) from three experts to assess expert and trainee differences and compute automated and expert assessed learning curves.
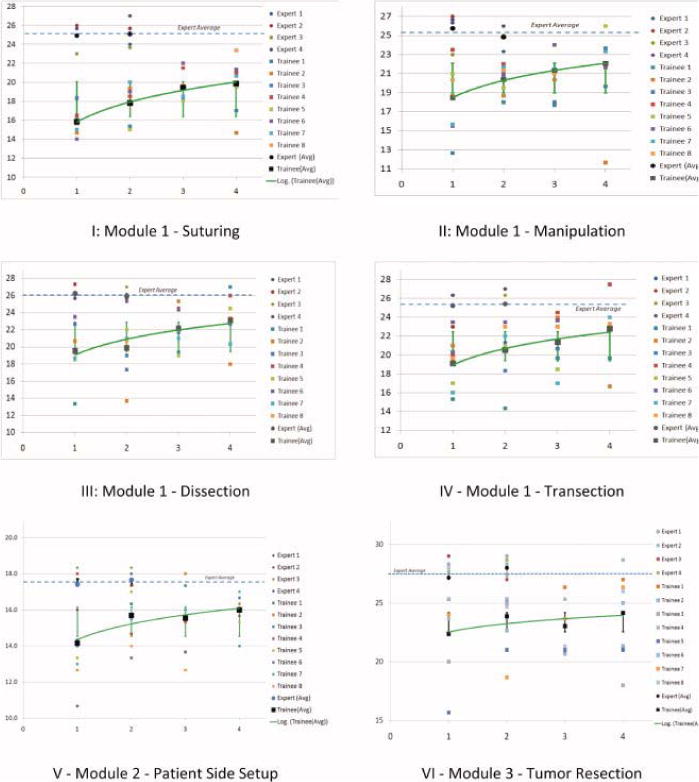
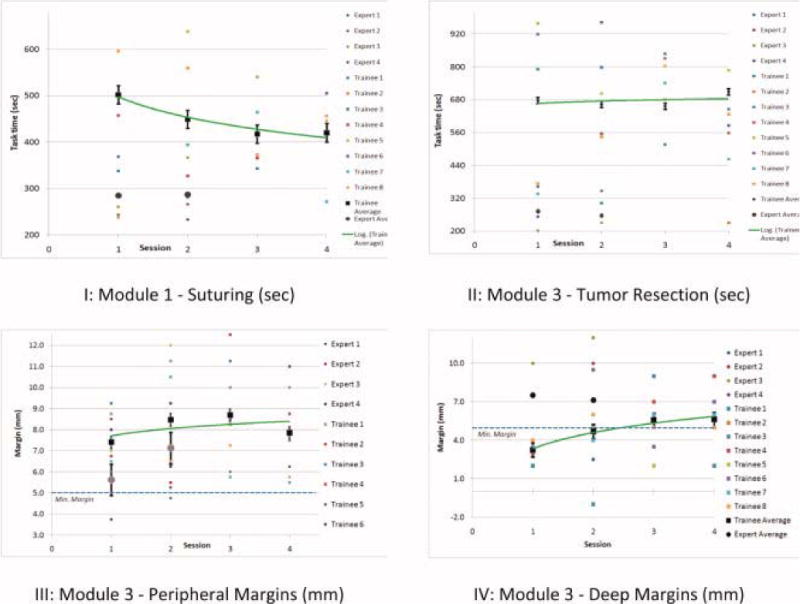
Results: Our data show that such training results in an improved didactic robotic knowledge base and improved clinical efficiency with respect to the set up and console manipulation. Experts (e.g., average OSATS, 25; standard deviation [SD], 3.1; module 1, suturing) and trainees (average OSATS, 15.9; SD, 3.9; week 1) are well separated at the beginning of the training, and the separation reduces significantly (expert average OSATS, 27.6; SD, 2.7; trainee average OSATS, 24.2; SD, 6.8; module 3) at the conclusion of the training. Learning curves in each of the three stages show diminishing differences between the experts and trainees, which is also consistent with expert assessment. Subjective assessment by experts verified the clinical utility of the module 3 surgical environment, and a survey of trainees consistently rated the curriculum as very useful in progression to human operating room assistance.
Conclusions: Structured curricular robotic surgery training with objective assessment promises to reduce the overhead for mentors, allow detailed assessment of human-machine interface skills, and create customized training models for individualized training. This preliminary study verifies the utility of such training in improving human-machine operations skills (module 1), and operating room and surgical skills (modules 2 and 3). In contrast to current coarse measures of total operating time and subjective assessment of error for short mass training sessions, these methods may allow individual tasks to be removed from the trainee regimen when skill levels are within the standard deviation of the experts for these tasks, which can greatly enhance overall efficiency of the training regimen and allow time for additional and more complex training to be incorporated in the same time frame.
Copyright © 2012 The American Laryngological, Rhinological, and Otological Society, Inc.
Figures
Comment in
-
In response to Objective assessment in residency-based training for transoral robotic surgery.Laryngoscope. 2013 May;123(5):1317. doi: 10.1002/lary.23960. Epub 2013 Feb 12. Laryngoscope. 2013. PMID: 23404291 No abstract available.
-
In reference to Objective assessment in residency-based training for transoral robotic surgery.Laryngoscope. 2013 May;123(5):1316. doi: 10.1002/lary.23920. Laryngoscope. 2013. PMID: 23619623 No abstract available.
Similar articles
-
In reference to Objective assessment in residency-based training for transoral robotic surgery.Laryngoscope. 2013 May;123(5):1316. doi: 10.1002/lary.23920. Laryngoscope. 2013. PMID: 23619623 No abstract available.
-
In response to Objective assessment in residency-based training for transoral robotic surgery.Laryngoscope. 2013 May;123(5):1317. doi: 10.1002/lary.23960. Epub 2013 Feb 12. Laryngoscope. 2013. PMID: 23404291 No abstract available.
-
Initial and Long-term Retention of Robotic Technical Skills in an Otolaryngology Residency Program.Laryngoscope. 2019 Jun;129(6):1380-1385. doi: 10.1002/lary.27425. Epub 2018 Aug 10. Laryngoscope. 2019. PMID: 30098045
-
Transoral Robotic Surgical Proficiency Via Real-Time Tactile Collision Awareness System.Laryngoscope. 2020 Dec;130 Suppl 6:S1-S17. doi: 10.1002/lary.29034. Epub 2020 Aug 31. Laryngoscope. 2020. PMID: 32865822
-
Robotic Surgery: The Impact of Simulation and Other Innovative Platforms on Performance and Training.J Minim Invasive Gynecol. 2021 Mar;28(3):490-495. doi: 10.1016/j.jmig.2020.12.001. Epub 2020 Dec 10. J Minim Invasive Gynecol. 2021. PMID: 33310145 Review.
Cited by
-
Using virtual reality to maintain surgical skills during periods of robotic surgery inactivity.J Robot Surg. 2014 Sep;8(3):261-8. doi: 10.1007/s11701-014-0465-0. Epub 2014 Apr 29. J Robot Surg. 2014. PMID: 27637688
-
Training in robotic-assisted surgery: a systematic review of training modalities and objective and subjective assessment methods.Surg Endosc. 2024 Jul;38(7):3547-3555. doi: 10.1007/s00464-024-10915-7. Epub 2024 May 30. Surg Endosc. 2024. PMID: 38814347 Free PMC article.
-
Toward Intraoperative Image-Guided Transoral Robotic Surgery.J Robot Surg. 2013 Sep;7(3):217-25. doi: 10.1007/s11701-013-0420-5. J Robot Surg. 2013. PMID: 25525474 Free PMC article.
-
Image-based and textbook-based virtual reality training on operational skills among junior residents: a proof of concept study.BMC Med Educ. 2025 May 7;25(1):668. doi: 10.1186/s12909-025-07245-0. BMC Med Educ. 2025. PMID: 40336062 Free PMC article. Clinical Trial.
-
Introductory TORS training in an otolaryngology residency program.J Robot Surg. 2018 Dec;12(4):617-623. doi: 10.1007/s11701-018-0784-7. Epub 2018 Feb 7. J Robot Surg. 2018. PMID: 29417393
References
-
- Parsons JT, et al. Squamous cell carcinoma of the oropharynx: surgery, radiation therapy, or both. Cancer. 2002;94(11):2967–80. - PubMed
-
- McLeod IK, Mair EA, Melder PC. Potential applications of the da Vinci minimally invasive surgical robotic system in otolaryngology. Ear Nose Throat J. 2005;84(8):483–7. - PubMed
-
- McLeod IK, Melder PC. Da Vinci robot-assisted excision of a vallecular cyst: a case report. Ear Nose Throat J. 2005;84(3):170–2. - PubMed
-
- Cohen MA, et al. Transoral robotic surgery and human papillomavirus status: Oncologic results. Head Neck. 33(4):573–80. - PubMed
-
- Genden EM, et al. The role of reconstruction for transoral robotic pharyngectomy and concomitant neck dissection. Arch Otolaryngol Head Neck Surg. 137(2):151–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
