

Epigenetic therapy using belinostat for patients with unresectable hepatocellular carcinoma: a multicenter phase I/II study with biomarker and pharmacokinetic analysis of tumors from patients in the Mayo Phase II Consortium and the Cancer Therapeutics Research Group
- PMID: 22915658
- PMCID: PMC3438233
- DOI: 10.1200/JCO.2011.41.2395
Epigenetic therapy using belinostat for patients with unresectable hepatocellular carcinoma: a multicenter phase I/II study with biomarker and pharmacokinetic analysis of tumors from patients in the Mayo Phase II Consortium and the Cancer Therapeutics Research Group
Abstract
Purpose: Epigenetic aberrations have been reported in hepatocellular carcinoma (HCC). In this study of patients with unresectable HCC and chronic liver disease, epigenetic therapy with the histone deacetylase inhibitor belinostat was assessed. The objectives were to determine dose-limiting toxicity and maximum-tolerated dose (MTD), to assess pharmacokinetics in phase I, and to assess activity of and explore potential biomarkers for response in phase II.
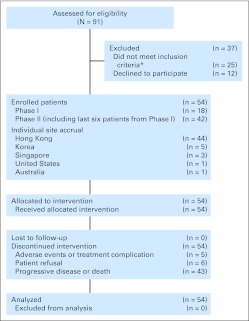
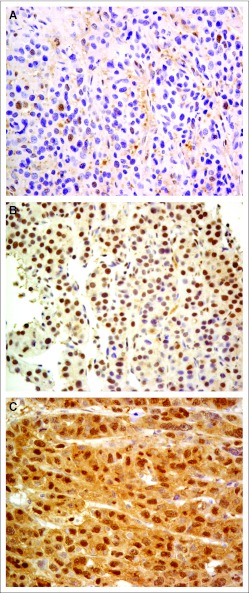
Patients and methods: Major eligibility criteria included histologically confirmed unresectable HCC, European Cooperative Oncology Group performance score ≤ 2, and adequate organ function. Phase I consisted of 18 patients; belinostat was given intravenously once per day on days 1 to 5 every 3 weeks; dose levels were 600 mg/m(2) per day (level 1), 900 mg/m(2) per day (level 2), 1,200 mg/m(2) per day (level 3), and 1,400 mg/m(2) per day (level 4). Phase II consisted of 42 patients. The primary end point was progression-free survival (PFS), and the main secondary end points were response according to Response Evaluation Criteria in Solid Tumors (RECIST) and overall survival (OS). Exploratory analysis was conducted on pretreatment tumor tissues to determine whether HR23B expression is a potential biomarker for response.
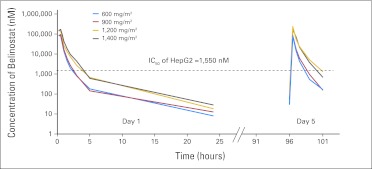
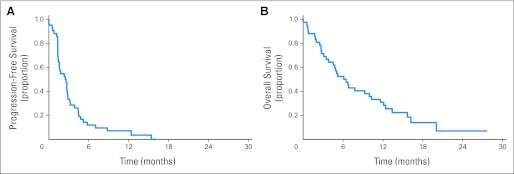
Results: Belinostat pharmacokinetics were linear from 600 to 1,400 mg/m(2) without significant accumulation. The MTD was not reached at the maximum dose administered. Dose level 4 was used in phase II. The median number of cycles was two (range, one to 12). The partial response (PR) and stable disease (SD) rates were 2.4% and 45.2%, respectively. The median PFS and OS were 2.64 and 6.60 months, respectively. Exploratory analysis revealed that disease stabilization rate (complete response plus PR plus SD) in tumors having high and low HR23B histoscores were 58% and 14%, respectively (P = .036).
Conclusion: Epigenetic therapy with belinostat demonstrates tumor stabilization and is generally well-tolerated. HR23B expression was associated with disease stabilization.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378–390. - PubMed
-
- Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10:25–34. - PubMed
-
- Zhong S, Yeo W, Tang MW, et al. Intensive hypermethylation of the CpG island of Ras association domain family 1A in hepatitis B virus-associated hepatocellular carcinomas. Clin Cancer Res. 2003;9:3376–3382. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
