

Optimizing pain control through the use of implantable pumps
- PMID: 22915907
- PMCID: PMC3417909
- DOI: 10.2147/mder.s3623
Optimizing pain control through the use of implantable pumps
Abstract
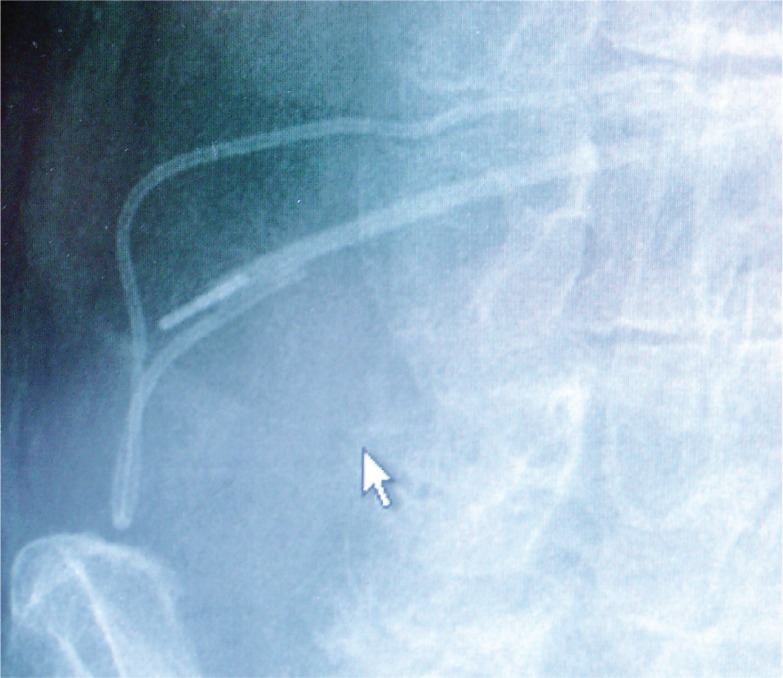
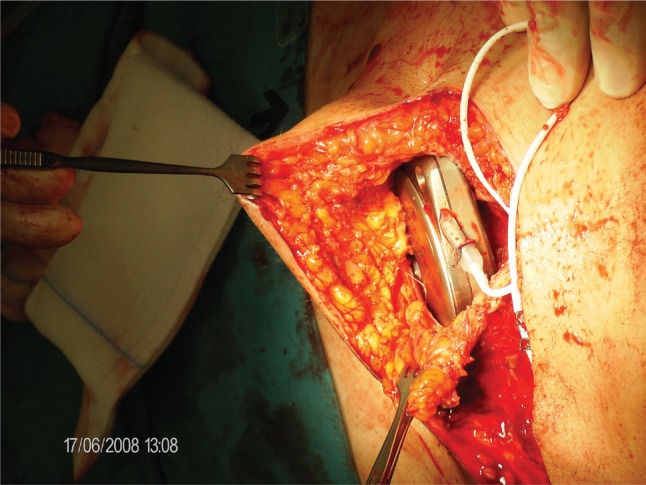
Intrathecal therapy represents an effective and well established treatment of nonmalignant as well as malignant pain. Devices available include mechanical constant flow pumps as well as electronic variable flow pumps with patient-controlled bolus release. The latter provide faster dose finding, individual pain control, and good acceptance by patients. New technologies such as membrane pumps and rechargeable devices are expected to be developed to clinical perfection. The available drugs for intrathecal therapy are listed according to the polyanalgesic consensus on intrathecal therapy. The integration of remote patient-controlled analgesia into electronic implantable devices, and the peptide analgesic ziconotide, have significantly improved intrathecal therapy. Complications include infections, catheter ruptures or disconnections, catheter granulomas, and technical dysfunctions. Further possibilities for optimizing intrathecal therapy include development of new drugs, drug side effects, catheter and pump technologies, and surgical techniques.
Keywords: implantable pumps; intrathecal catheters; intrathecal drugs; intrathecal pain control; intrathecal therapy; morphine pumps.
Figures

References
-
- Auroy Y, Narchi P, et al. Serious complications related to regional anesthesia: results of a prospective survey in France. Anesthesiology. 1997;87:479–86. - PubMed
-
- Bennett G, Burchiel K, et al. Clinical guidelines for intraspinal infusion: report of an expert panel. PolyAnalgesic Consensus Conference 2000. J Pain Symptom Manage. 2000;20:S37–43. - PubMed
-
- Chan VW, Garcia J, et al. A comparative study of low-dose hyperbaric spinal lidocaine 0.5% versus 5% for continuous spinal anesthesia. Reg Anesth Pain Med. 1998;23:164–9. - PubMed
-
- Coffey RJ, Burchiel K. Inflammatory mass lesions associated with intrathecal drug infusion catheters: report and observations on 41 patients. Neurosurgery. 2002;50:78–86. 86–7. discussion. - PubMed
-
- Dahm PO, Nitescu PV, et al. Six years of continuous intrathecal infusion of opioid and bupivacaine in the treatment of refractory pain due to intrapelvic extrusion of bone cement after total hip arthroplasty. Reg Anesth Pain Med. 1998;23:315–9. - PubMed
LinkOut - more resources
Full Text Sources
