

Multimodality imaging evaluation of functional and clinical benefits of percutaneous coronary intervention in patients with chronic total occlusion lesion
- PMID: 22916078
- PMCID: PMC3425125
- DOI: 10.7150/thno.4717
Multimodality imaging evaluation of functional and clinical benefits of percutaneous coronary intervention in patients with chronic total occlusion lesion
Abstract
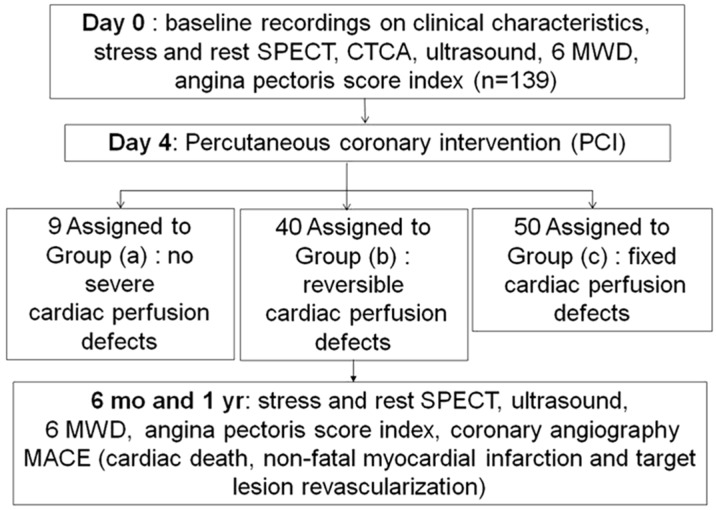
Aims: To determine the effects of percutaneous coronary intervention (PCI) on cardiac perfusion, cardiac function, and quality of life in patients with chronic total occlusion (CTO) lesion in left anterior descending (LAD) coronary artery.
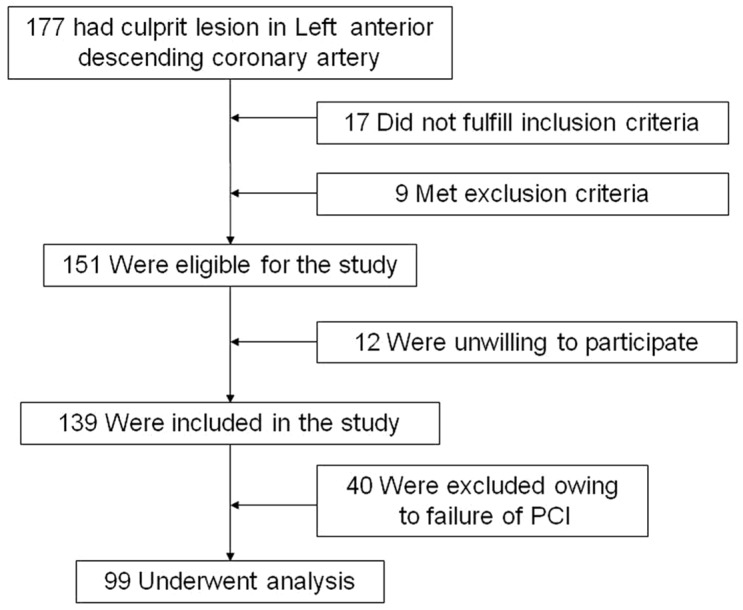
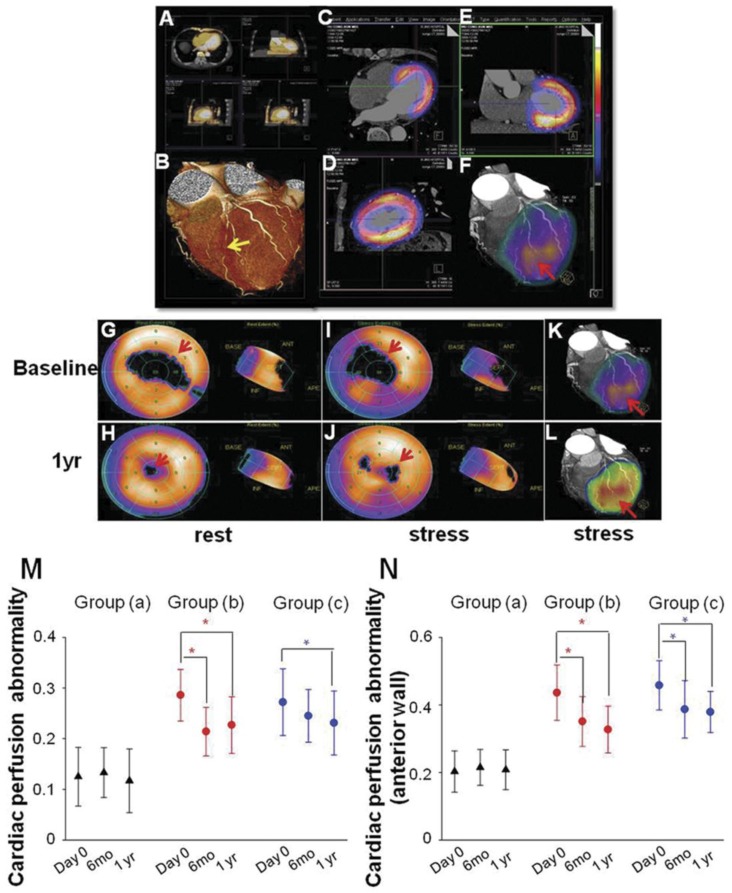
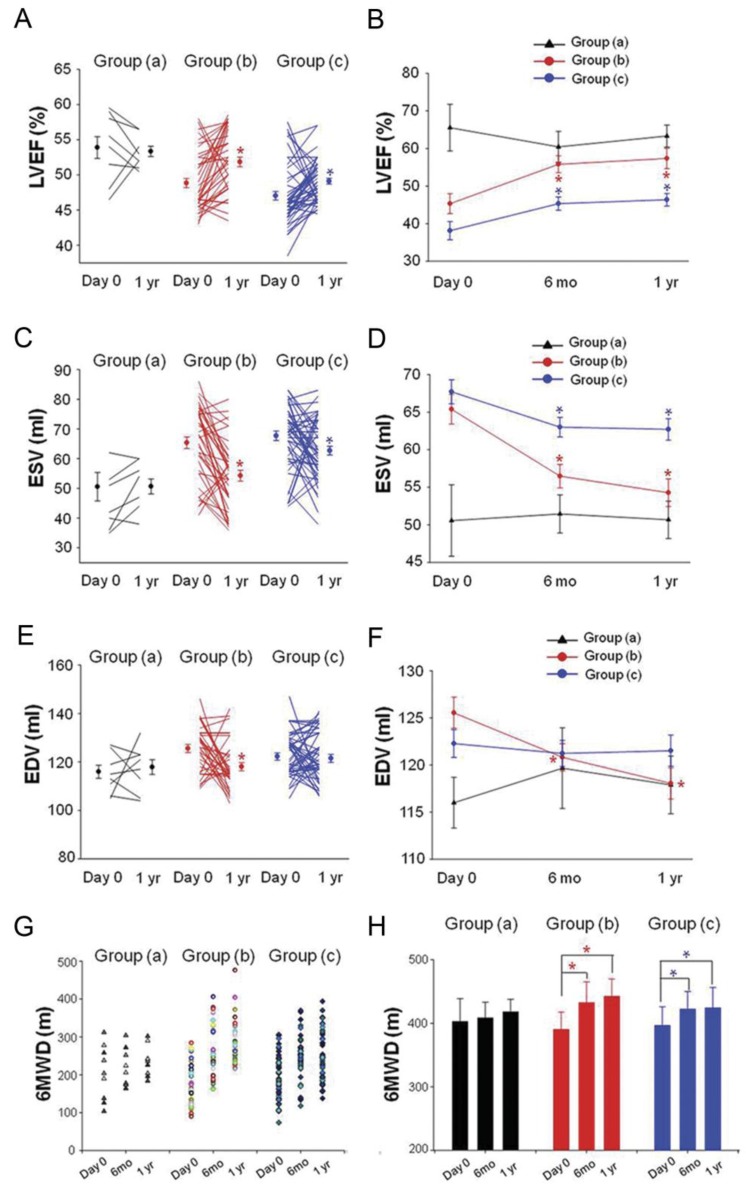
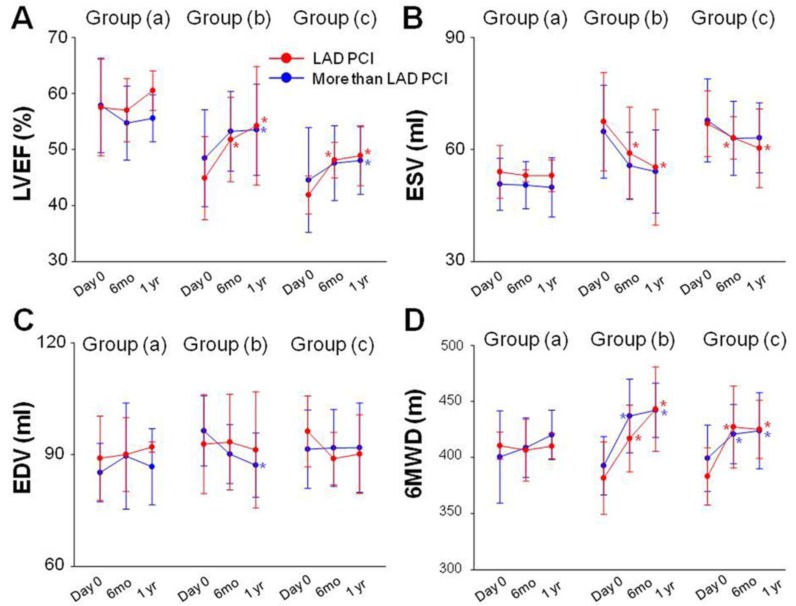
Methods and results: Patients (n=99) with CTO lesion in the LAD coronary artery who had successfully undergone PCI were divided into three groups based on the SPECT/CTCA fusion imaging: (a) no severe cardiac perfusion defects (n=9); (b) reversible cardiac perfusion defects (n=40); or (c) fixed cardiac perfusion defects (n=50). No statistical difference of perfusion abnormality was observed at 6 months and 1 year after PCI in group (a). In group (b), SPECT/CTCA fusion imaging demonstrated that cardiac perfusion abnormality was significantly decreased 6 month and 1 year after PCI. Left ventricular ejection fraction (LVEF) increased significantly at 6 months and 1 year follow up. Quality of life improved at 6 months and 1 year after PCI procedure. Moreover, patients in group (c) also benefited from PCI therapy: a decrease in cardiac perfusion abnormality, an increase in LVEF, and an improvement in quality of life. PCI of coronary arteries in addition to LAD did not significantly affect cardiac function and quality of life improvement in each group.
Conclusions: PCI exerts functional and clinical benefits in patients with CTO lesion in LAD coronary artery, particularly in patients with reversible cardiac perfusion defects. SPECT/CTCA fusion imaging may serve as a useful tool to evaluate the outcomes of patients with CTO lesion in LAD coronary artery.
Keywords: CTCA.; CTO; Chronic total occlusion; Computed tomography coronary angiography; PCI; Percutaneous coronary intervention; SPECT; Single-photon emission computed tomography.
Conflict of interest statement
Conflict of Interest: None declared.
Figures
References
-
- Christofferson RD, Lehmann KG, Martin GV. et al. Effect of chronic total coronary occlusion on treatment strategy. Am J Cardiol. 2005;95:1088–1091. - PubMed
-
- Kahn JK. Angiographic suitability for catheter revascularization of total coronary occlusions in patients from a community hospital setting. Am Heart J. 1993;126:561–564. - PubMed
-
- Berger AK, Edris DW, Breall JA. et al. Resource use and quality of care for Medicare patients with acute myocardial infarction in Maryland and the District of Columbia: analysis of data from the Cooperative Cardiovascular Project. Am Heart J. 1998;135:349–356. - PubMed
-
- Guadagnoli E, Hauptman PJ, Ayanian JZ. et al. Variation in the use of cardiac procedures after acute myocardial infarction. N Engl J Med. 1995;333:573–578. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
