

Therapeutic angiogenesis for treating cardiovascular diseases
- PMID: 22916079
- PMCID: PMC3425124
- DOI: 10.7150/thno.4419
Therapeutic angiogenesis for treating cardiovascular diseases
Abstract
Cardiovascular disease is the leading cause of death worldwide and is often associated with partial or full occlusion of the blood vessel network in the affected organs. Restoring blood supply is critical for the successful treatment of cardiovascular diseases. Therapeutic angiogenesis provides a valuable tool for treating cardiovascular diseases by stimulating the growth of new blood vessels from pre-existing vessels. In this review, we discuss strategies developed for therapeutic angiogenesis using single or combinations of biological signals, cells and polymeric biomaterials. Compared to direct delivery of growth factors or cells alone, polymeric biomaterials provide a three-dimensional drug-releasing depot that is capable of facilitating temporally and spatially controlled release. Biomimetic signals can also be incorporated into polymeric scaffolds to allow environmentally-responsive or cell-triggered release of biological signals for targeted angiogenesis. Recent progress in exploiting genetically engineered stem cells and endogenous cell homing mechanisms for therapeutic angiogenesis is also discussed.
Keywords: Angiogenesis; Cardiovascular Diseases.
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
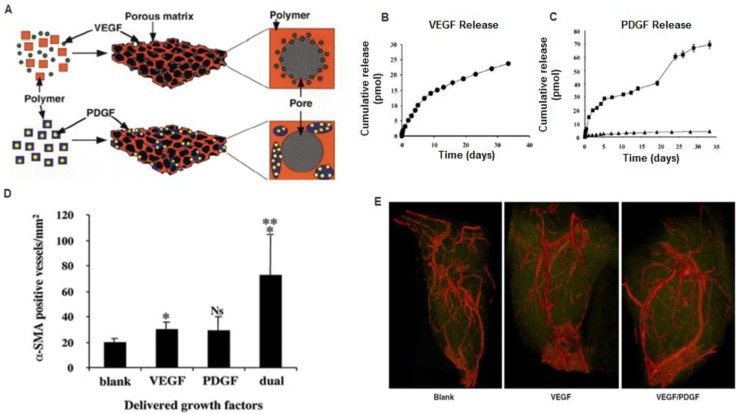
 75:25, intrinsic viscosity = 0.69 dl/g; 75:25,
75:25, intrinsic viscosity = 0.69 dl/g; 75:25,  intrinsic viscosity = 0.2 dl/g), before scaffold fabrication. D) Dual delivery led to early maturation of blood vessels as demonstrated by α-smooth muscle actin staining at 2 weeks. E) Representative micro-CT images after 5 weeks intramuscular injections of alginate (Blank), alginate containing VEGF165 (VEGF), or alginate containing VEGF165 combined with PLGA microspheres containing PDGF-BB (VEGF/PDGF).(A-D) Reproduced with permission from ref (E) Reproduced with permission from ref .
intrinsic viscosity = 0.2 dl/g), before scaffold fabrication. D) Dual delivery led to early maturation of blood vessels as demonstrated by α-smooth muscle actin staining at 2 weeks. E) Representative micro-CT images after 5 weeks intramuscular injections of alginate (Blank), alginate containing VEGF165 (VEGF), or alginate containing VEGF165 combined with PLGA microspheres containing PDGF-BB (VEGF/PDGF).(A-D) Reproduced with permission from ref (E) Reproduced with permission from ref .
References
-
- Libby P, Theroux P. Pathophysiology of coronary artery disease. Circulation. 2005;111(25):3481–8. - PubMed
-
- Jawad E, Arora R. Chronic stable angina pectoris. Dis Mon. 2008;54(9):671–89. - PubMed
-
- McFalls E.O. et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med. 2004;351(27):2795–804. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
