

Hepatitis C virus in Vietnam: high prevalence of infection in dialysis and multi-transfused patients involving diverse and novel virus variants
- PMID: 22916104
- PMCID: PMC3419252
- DOI: 10.1371/journal.pone.0041266
Hepatitis C virus in Vietnam: high prevalence of infection in dialysis and multi-transfused patients involving diverse and novel virus variants
Abstract
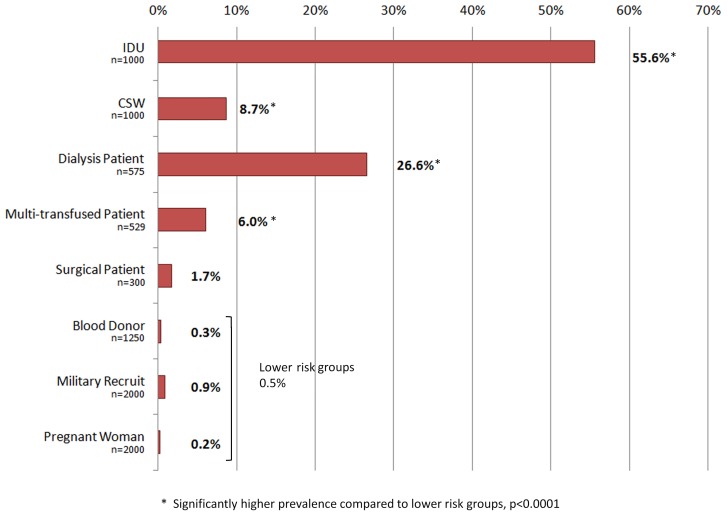
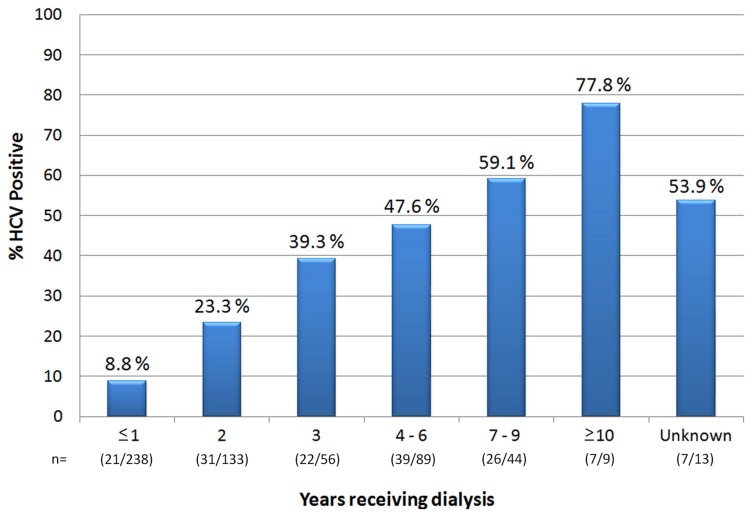
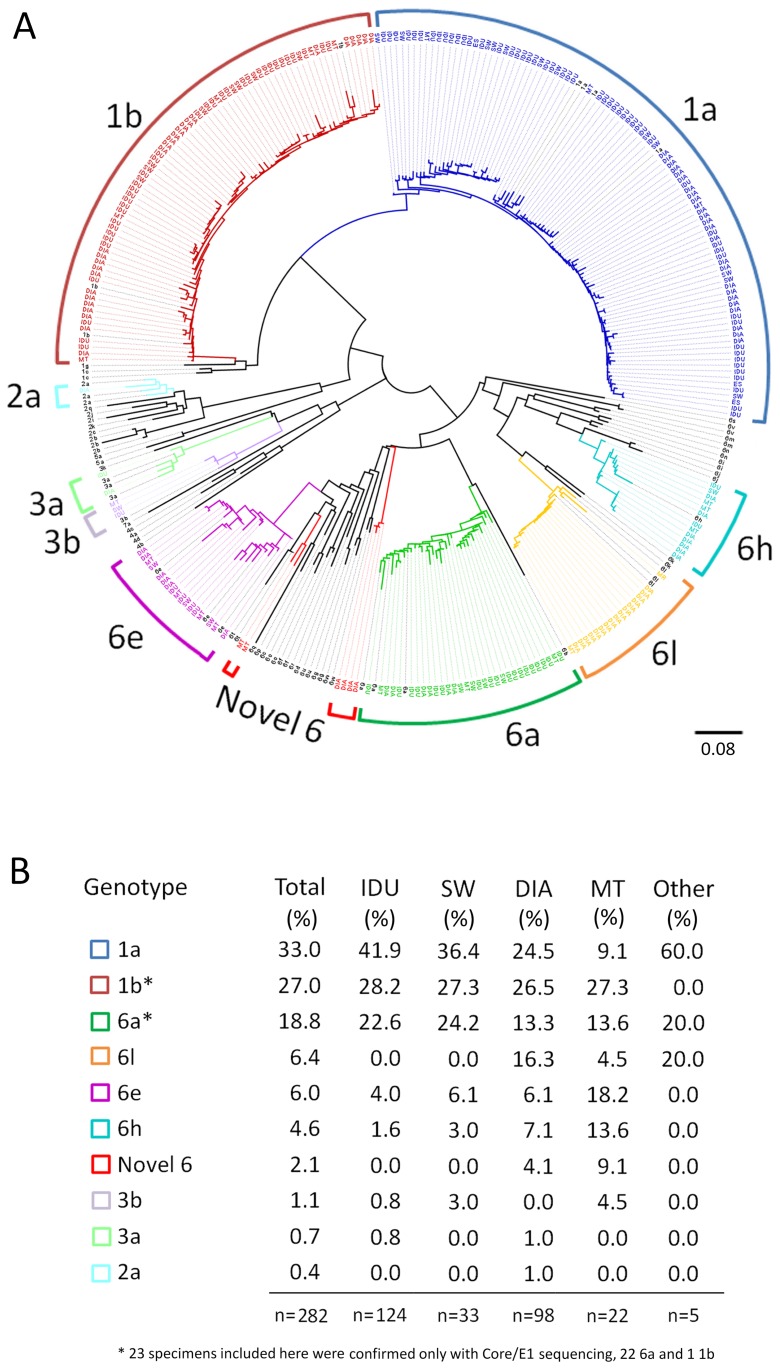
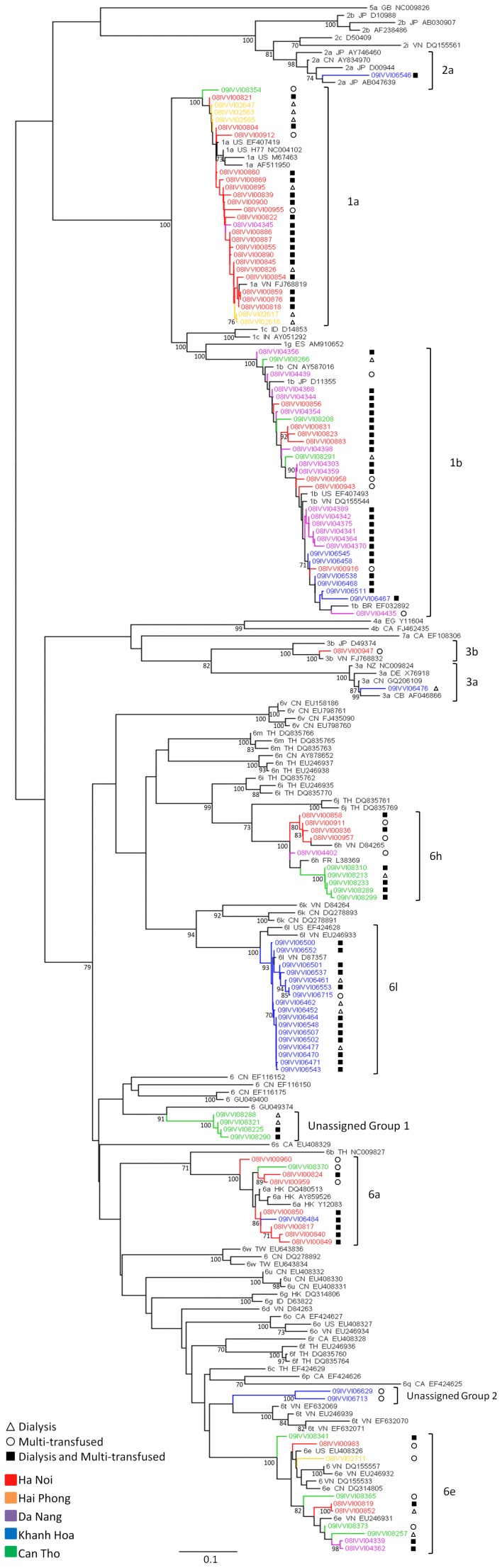
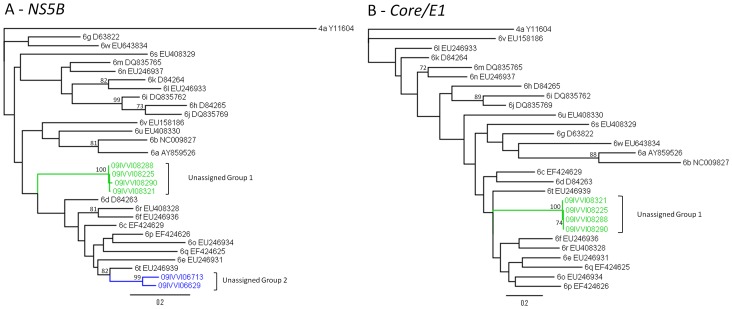
Hepatitis C virus (HCV) is a genetically diverse pathogen infecting approximately 2-3% of the world's population. Herein, we describe results of a large, multicentre serological and molecular epidemiological study cataloguing the prevalence and genetic diversity of HCV in five regions of Vietnam; Ha Noi, Hai Phong, Da Nang, Khanh Hoa and Can Tho. Individuals (n=8654) with varying risk factors for infection were analysed for the presence of HCV Ab/Ag and, in a subset of positive specimens, for HCV RNA levels (n=475) and genotype (n=282). In lower risk individuals, including voluntary blood donors, military recruits and pregnant women, the prevalence of infection was 0.5% (n=26/5250). Prevalence rates were significantly higher (p<0.001) in intravenous drug users (IDUs; 55.6%, n=556/1000), dialysis patients (26.6%, n=153/575) commercial sex workers (CSWs; 8.7%, n=87/1000), and recipients of multiple blood transfusions (6.0%, n=32/529). The prevalence of HCV in dialysis patients varied but remained high in all regions (11-43%) and was associated with the receipt of blood transfusions [OR: 2.08 (1.85-2.34), p=0.001], time from first transfusion [OR: 1.07 (1.01-1.13), p=0.023], duration of dialysis [OR: 1.31 (1.19-1.43), p<0.001] and male gender [OR: 1.60 (1.06-2.41), p=0.026]. Phylogenetic analysis revealed high genetic diversity, particularly amongst dialysis and multi-transfused patients, identifying subtypes 1a (33%), 1b (27%), 2a (0.4%), 3a (0.7%), 3b (1.1%), 6a (18.8%), 6e (6.0%), 6h (4.6%), 6l (6.4%) and 2 clusters of novel genotype 6 variants (2.1%). HCV genotype 1 predominated in Vietnam (60%, n=169/282) but the proportion of infections attributable to genotype 1 varied between regions and risk groups and, in the Southern part of Vietnam, genotype 6 viruses dominated in dialysis and multi-transfused patients (73.9%). This study confirms a high prevalence of HCV infection in Vietnamese IDUs and, notably, reveals high levels of HCV infection associated with dialysis and blood transfusion.
Conflict of interest statement
Figures
Similar articles
-
Multiple routes of hepatitis C virus transmission among injection drug users in Hai Phong, Northern Vietnam.J Med Virol. 2010 Aug;82(8):1355-63. doi: 10.1002/jmv.21787. J Med Virol. 2010. PMID: 20572071
-
Epidemiological distribution and genotype characterization of hepatitis C virus and HIV co-infection in Wuhan, China, where the prevalence of HIV is low.J Med Virol. 2013 Oct;85(10):1712-23. doi: 10.1002/jmv.23650. Epub 2013 Jul 19. J Med Virol. 2013. PMID: 23868809
-
A multicentre molecular analysis of hepatitis B and blood-borne virus coinfections in Viet Nam.PLoS One. 2012;7(6):e39027. doi: 10.1371/journal.pone.0039027. Epub 2012 Jun 13. PLoS One. 2012. PMID: 22720022 Free PMC article.
-
Hepatitis C Virus in mainland China with an emphasis on genotype and subtype distribution.Virol J. 2017 Feb 23;14(1):41. doi: 10.1186/s12985-017-0710-z. Virol J. 2017. PMID: 28231805 Free PMC article. Review.
-
Genetic history of hepatitis C virus genotype 6 in Taiwan.J Formos Med Assoc. 2024 Sep;123(9):926-933. doi: 10.1016/j.jfma.2023.10.013. Epub 2023 Nov 22. J Formos Med Assoc. 2024. PMID: 37996321 Review.
Cited by
-
Prevalence and genotype distribution of hepatitis C virus within hemodialysis units in Thailand: role of HCV core antigen in the assessment of viremia.BMC Infect Dis. 2022 Jan 22;22(1):79. doi: 10.1186/s12879-022-07074-2. BMC Infect Dis. 2022. PMID: 35065604 Free PMC article.
-
Robust and persistent replication of the genotype 6a hepatitis C virus replicon in cell culture.Antimicrob Agents Chemother. 2014 May;58(5):2638-46. doi: 10.1128/AAC.01780-13. Epub 2014 Feb 18. Antimicrob Agents Chemother. 2014. PMID: 24550344 Free PMC article.
-
Evolving Diversity of Hepatitis C Viruses in Yunnan Honghe, China.Int J Mol Sci. 2016 Mar 18;17(3):403. doi: 10.3390/ijms17030403. Int J Mol Sci. 2016. PMID: 26999127 Free PMC article.
-
Genotype and genetic variation of HCV infections with low-risk factors in Putian coastal regions, China.Epidemiol Infect. 2017 Dec;145(16):3385-3397. doi: 10.1017/S0950268817002357. Epub 2017 Oct 30. Epidemiol Infect. 2017. PMID: 29081304 Free PMC article.
-
Conservation in China of a novel group of HCV variants dating to six centuries ago.Virology. 2014 Sep;464-465:21-25. doi: 10.1016/j.virol.2014.06.011. Epub 2014 Jul 18. Virology. 2014. PMID: 25043585 Free PMC article.
References
-
- Shepard CW, Finelli L, Alter MJ (2005) Global epidemiology of hepatitis C virus infection. The Lancet infectious diseases 5: 558–567. - PubMed
-
- Perz JFFL, Pecoraro C, Hutin YJF, Armstrong GL (2004) Estimated global prevalence of hepatitis C virus infection. 42nd Annual Meeting of the Infectious Disease Soceity of America; Boston, MA, USA Sept 30–Oct 3.
-
- World Health Organisation (2000) Hepatitis C–global prevalence (update). Weekly epidemiological record/Health Section of the Secretariat of the League of Nations 75: 18–19.
-
- Sievert W, Altraif I, Razavi HA, Abdo A, Ahmed EA, et al. (2011) A systematic review of hepatitis C virus epidemiology in Asia, Australia and Egypt. Liver international : official journal of the International Association for the Study of the Liver 31 Suppl 2: 61–80. - PubMed
-
- Alter MJ (2011) HCV routes of transmission: what goes around comes around. Seminars in liver disease 31: 340–346. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
