

Tips and tricks in the dermoscopy of pigmented lesions
- PMID: 22916721
- PMCID: PMC3519649
- DOI: 10.1186/1471-5945-12-14
Tips and tricks in the dermoscopy of pigmented lesions
Abstract
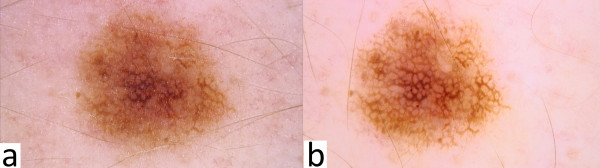
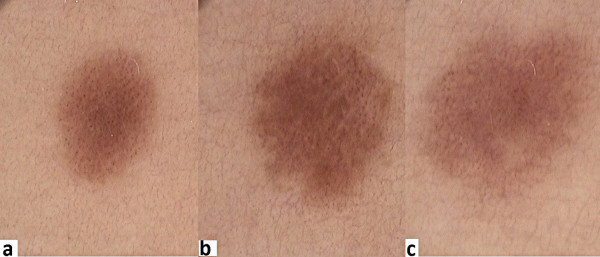
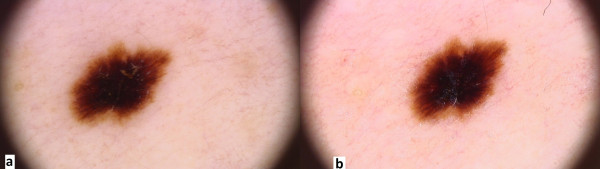
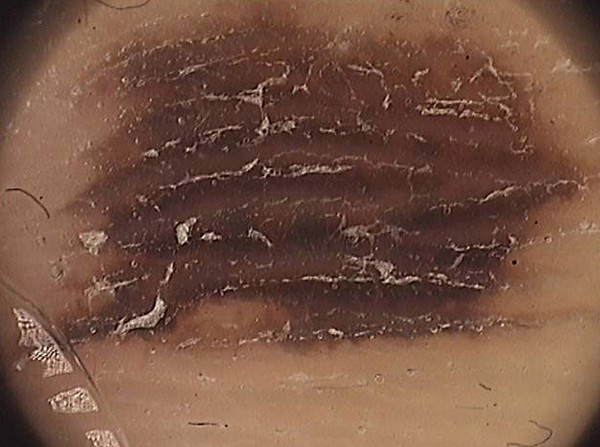
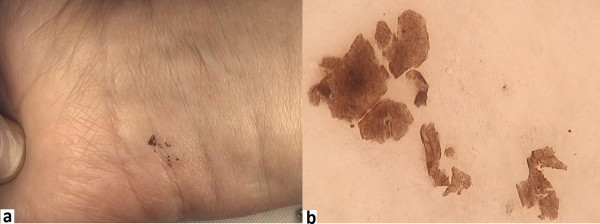
Dermoscopy is a useful, widely used tool for examining pigmented lesions, especially helpful in cases of an uncertain nature. Nevertheless, doctors may experience diagnostic difficulties while using this method. An example of this may be found in the examination of subcorneal hematoma, dark nevi with black lamella or lesions of acral volar skin. In such cases, a few diagnostic tricks have proven to be helpful in achieving diagnostic accuracy. This paper reviews various methods of performing dermoscopy, suggesting a number of simple, yet helpful tests. These include the adhesive tape test, the skin scraping test and the ink furrow test. The adhesive tape test is helpful in differentiating between dark melanocytic nevi and melanoma. Hematoma may be more easily differentiated with the use of the so-called skin scraping test. The confirmation of benign and melanocytic lesions of acral volar skin, on the other hand, is more accurate when using the ink furrow test. These methods have been discussed here based upon a series of literature reviews, the authors' own experience and, also, iconography. The present article describes novel methods used in dermoscopy, helping to bring about a faster, more accurate diagnostics of those lesions which have proven to be more difficult to recognize. Helpful tricks, such as have been known to professional literature, as well as the authors' own experience (for instance, applying urea cream to hyperkeratotic lesions or using photographs of skin lesions taken with the aid of a mobile phone camera--all prior to surgery) will surely be considered beneficial to the practitioner, be it dermatologist or any other physician.
Figures



References
-
- Zalaudek I, Kittler H, Marghoob AA, Balato A, Blum A, Dalle S, Ferrara G, Fink-Puches R, Giorgio CM, Hofmann-Wellenhof R, Malvehy J, Moscarella E, Puig S, Scalvenzi M, Thomas L, Argenziano G. Time required for a complete skin examination with and without dermoscopy: a prospective, randomized multicenter study. Arch Dermatol. 2008;144:509–513. doi: 10.1001/archderm.144.4.509. - DOI - PubMed
-
- Seidenari S, Pellacani G, Martella A, Giusti F, Argenziano G, Buccini P, Carli P, Catricalà C, De Giorgi V, Ferrari A, Ingordo V, Manganoni AM, Peris K, Piccolo D, Pizzichetta MA. Instrument-, age- and site-dependent variations of dermoscopic patterns of congenital melanocytic naevi: a multicentre study. Br J Dermatol. 2006;155:56–61. doi: 10.1111/j.1365-2133.2006.07182.x. - DOI - PubMed
-
- Ruocco E, Argenziano G, Pellacani G, Seidenari S. Noninvasive imaging of skin tumors. Dermatol Surg. 2004;30(2 Pt 2):301–310. - PubMed
-
- Kaminska-Winciorek G, Spiewak R. Basic dermoscopy of melanocytic lesions for beginners. Postepy Hig Med Dosw (Online) 2011;65:501–508. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
