

Parietal epithelial cell activation marker in early recurrence of FSGS in the transplant
- PMID: 22917699
- PMCID: PMC3488951
- DOI: 10.2215/CJN.10571011
Parietal epithelial cell activation marker in early recurrence of FSGS in the transplant
Abstract
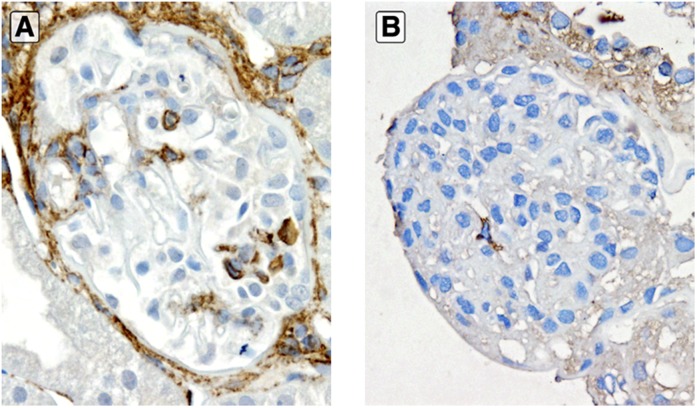
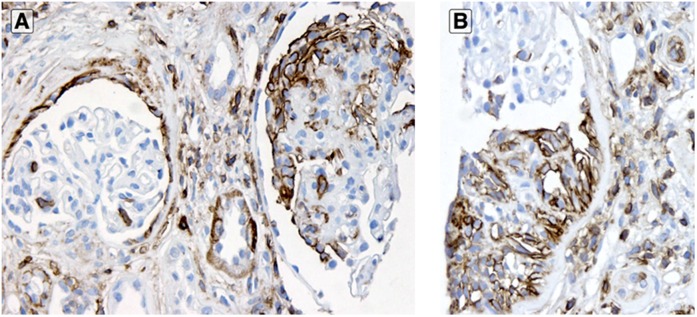
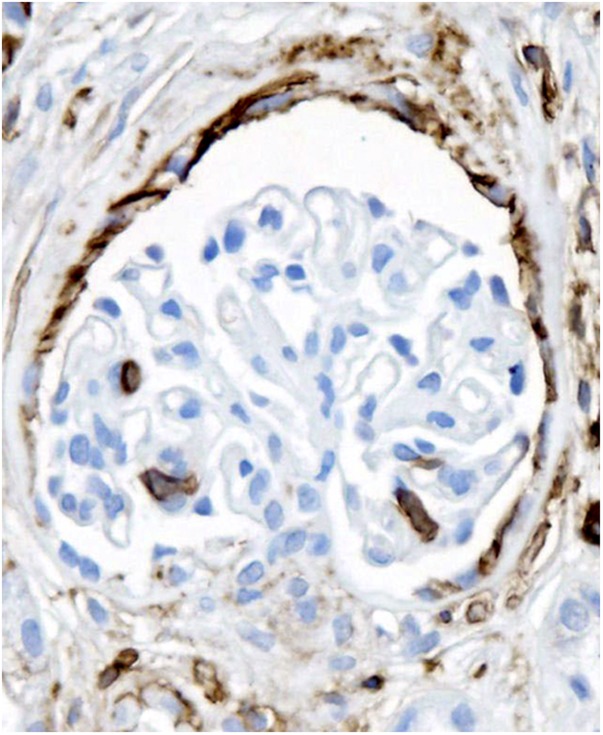
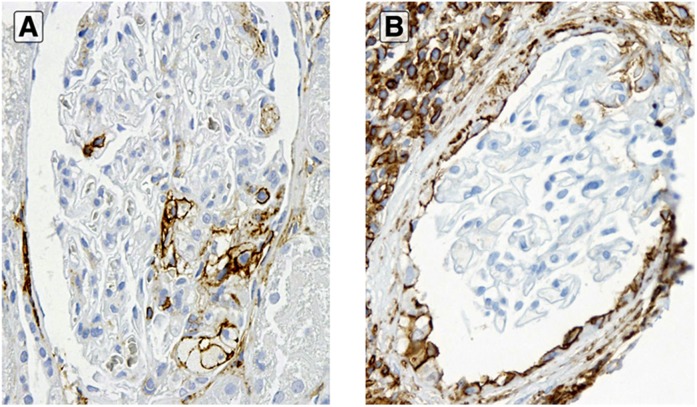
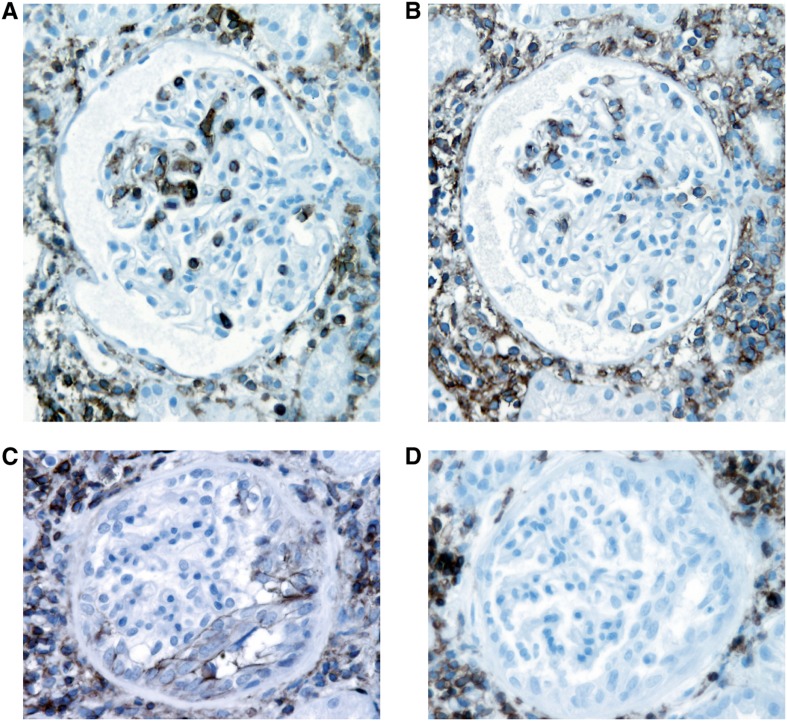
Background and objectives: Podocyte loss is key in glomerulosclerosis. Activated parietal epithelial cells are proposed to contribute to pathogenesis of glomerulosclerosis and may serve as stem cells that can transition to podocytes. CD44 is a marker for activated parietal epithelial cells. This study investigated whether activated parietal epithelial cells are increased in early recurrent FSGS in transplant compared with minimal change disease.
Design, setting, participants, & measurements: CD44 staining in renal allograft biopsies from 12 patients with recurrent FSGS was performed and compared with native kidneys with minimal change disease or FSGS and normal control native and transplant kidneys without FSGS. CD44+ epithelial cells along Bowman's capsule in the parietal epithelial cell location and over the glomerular tuft in the visceral epithelial cell location were assessed.
Results: Cases with early recurrent FSGS manifesting only foot process effacement showed significantly increased CD44+ visceral epithelial cells involving 29.0% versus 2.6% of glomeruli in minimal change disease and 0% in non-FSGS transplants. Parietal location CD44 positivity also was numerically increased in recurrent FSGS. In later transplant biopsies, glomeruli with segmental lesions had more CD44+ visceral epithelial cells than glomeruli without lesions.
Conclusions: Parietal epithelial cell activation marker is significantly increased in evolving FSGS versus minimal change disease, and this increase may distinguish early FSGS from minimal change disease. Whether parietal epithelial cell activation contributes to pathogenesis of sclerosis in idiopathic FSGS or is a regenerative/repair response to replace injured podocytes awaits additional study.
Figures
References
-
- Fogo AB: Minimal change disease and focal segmental glomerulosclerosis. In: Fundamentals of Renal Pathology, edited by Fogo AB, New York, Springer Science, 2005, pp 40–52
-
- Haas M, Meehan SM, Karrison TG, Spargo BH: Changing etiologies of unexplained adult nephrotic syndrome: A comparison of renal biopsy findings from 1976-1979 and 1995-1997. Am J Kidney Dis 30: 621–631, 1997 - PubMed
-
- Braden GL, Mulhern JG, O’Shea MH, Nash SV, Ucci AA, Jr, Germain MJ: Changing incidence of glomerular diseases in adults. Am J Kidney Dis 35: 878–883, 2000 - PubMed
-
- Dijkman H, Smeets B, van der Laak J, Steenbergen E, Wetzels J: The parietal epithelial cell is crucially involved in human idiopathic focal segmental glomerulosclerosis. Kidney Int 68: 1562–1572, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
