

Armodafinil for sarcoidosis-associated fatigue: a double-blind, placebo-controlled, crossover trial
- PMID: 22917711
- PMCID: PMC3678278
- DOI: 10.1016/j.jpainsymman.2012.02.016
Armodafinil for sarcoidosis-associated fatigue: a double-blind, placebo-controlled, crossover trial
Abstract
Context: Fatigue has been identified in more than one-half of patients with sarcoidosis. Although fatigue is not synonymous with impaired quality of life, most studies of sarcoidosis identify fatigue as a major cause of impaired quality of life.
Objectives: To test the hypothesis that stimulants may have a role in the treatment of fatigued sarcoidosis patients, even without objective evidence of daytime sleepiness.
Methods: This was a double-blind, placebo-controlled, crossover study of sarcoidosis patients followed up in one sarcoidosis clinic Sarcoidosis patients with fatigue received either armodafinil or placebo with eight weeks of therapy for each arm and a two week washout period before crossover to the other treatment. Initial armodafinil dose was 150mg and increased to 250mg after four weeks. Patients underwent polysomnography and multiple sleep latency testing (MSLT) the following day. Patients with an apnea/hypopnea index <6/hour received either armodafinil or placebo. Polysomnography with MSLT was repeated after each treatment arm.
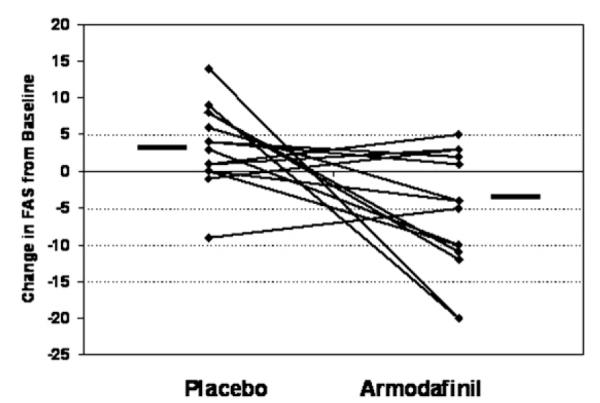
Results: Fifteen patients received the study drug. Fatigue was assessed using the Fatigue Assessment Scale (the lower the score, the less the fatigue) and the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) (the higher the score, the less the fatigue). After eight weeks of therapy, there was a significant improvement in the Fatigue Assessment Scale during armodafinil treatment (median -4.5, range -20, 5) compared with placebo treatment (median 3.5, range -9, 14, P<0.05) and for the FACIT-F (armodafinil: median 9, range -12, 26 vs. placebo: median -5, range -17, 11, P<0.005). This improvement in fatigue was seen for both those with and without shortened sleep onset latency time during the MSLT.
Conclusion: Armodafinil treatment led to a significant reduction in fatigue in sarcoidosis patients. This effect was seen even in patients who did not have excessive daytime somnolence.
Copyright © 2013 U.S. Cancer Pain Relief Committee. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- de Kleijn WP, de Vries J, Lower EE, et al. Fatigue in sarcoidosis: a systematic review. Curr Opin Pulm Med. 2009;15:499–506. - PubMed
-
- de Vries J, Rothkrantz-Kos S, Dieijen-Visser MP, Drent M. The relationship between fatigue and clinical parameters in pulmonary sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2004;21:127–136. - PubMed
-
- de Vries J, Michielsen H, van Heck GL, Drent M. Measuring fatigue in sarcoidosis: the Fatigue Assessment Scale (FAS) Br J Health Psychol. 2004;9(Pt 3):279–291. - PubMed
-
- de Kleijn WP, Elfferich MD, de Vries J, et al. Fatigue in sarcoidosis: American versus Dutch patients. Sarcoidosis Vasc Diffuse Lung Dis. 2009;26:92–97. - PubMed
-
- Gvozdenovic BS, Mihailovic-Vucinic V, Ilic-Dudvarski A, Zugic V, Judson MA. Differences in symptom severity and health status impairment between patients with pulmonary and pulmonary plus extrapulmonary sarcoidosis. Respir Med. 2008;102:1636–1642. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
