

Delayed recognition of diaphragmatic injury caused by penetrating thoraco-abdominal trauma
- PMID: 22918082
- PMCID: PMC3437398
- DOI: 10.1016/j.ijscr.2012.07.011
Delayed recognition of diaphragmatic injury caused by penetrating thoraco-abdominal trauma
Abstract
Introduction: Penetrating trauma to the thoraco-abdomen may cause diaphragmatic injury (DI). We present a case which highlights the difficulties of recognizing DI and the limited role of multimodal diagnostic imaging.
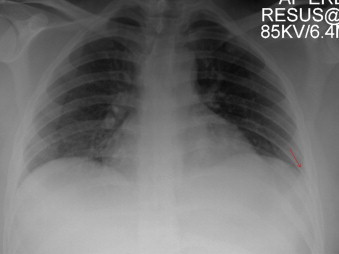
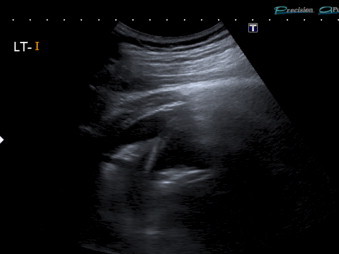
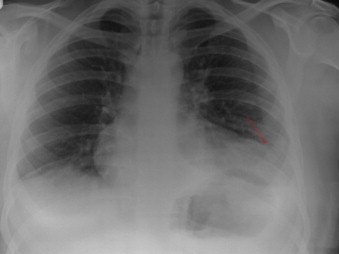
Presentation of case: A 19 year old male presented with stab wounds to his left lateral chest wall. CT was suspicious for diaphragmatic injury but this could not be confirmed despite ultrasound and serial plain radiographs. He was discharged but re-presented with respiratory compromise and diaphragmatic herniation.
Discussion: We review the clinical features of diaphragmatic injury after penetrating thoraco-abdominal trauma and the various imaging modalities available to clinicians.
Conclusion: A high index of suspicion must be employed for DI in the context of penetrating thoraco-abdominal trauma. Inpatient observation and laparoscopy/thoracoscopy should be considered when radiological findings are ambiguous. Front line physicians should also consider diaphragmatic herniation in stab victims who re-present with respiratory, circulatory, or gastrointestinal symptomology.
Copyright © 2012 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
Figures


References
-
- Berman G. House of Commons Library; London: 2011. Knife crime statistics. SN/SG/4304. Available at www.publications.parliament.uk/pa/cm200809/cmselect/cmhaff/112/11206.htm [accessed 06.03.12]
-
- Hospital Episode Statistics. The Health and Social Care Information Centre. National Health Service. Available at www.hesonline.nhs.uk [accessed 06.03.12].
-
- Williams M., Carlin A.M., Tyburski J.G., Blocksom J.M., Harvey E.H., Steffes C.P. Predictors of mortality in patients with traumatic diaphragmatic rupture and associated thoracic and/or abdominal injuries. American Surgeon. 2004;70(2):157–162. - PubMed
-
- Petrone P., Leppaniemi A., Inaba K., Soreide K., Asensio J.A. Diaphragmatic injuries: challenges in the diagnosis and management. Trauma. 2007;9:227–236.
LinkOut - more resources
Full Text Sources
Research Materials
