

Association between coronary vascular dysfunction and cardiac mortality in patients with and without diabetes mellitus
- PMID: 22919001
- PMCID: PMC3495105
- DOI: 10.1161/CIRCULATIONAHA.112.120402
Association between coronary vascular dysfunction and cardiac mortality in patients with and without diabetes mellitus
Abstract
Background: Diabetes mellitus increases the risk of adverse cardiac outcomes and is considered a coronary artery disease (CAD) equivalent. We examined whether coronary vascular dysfunction, an early manifestation of CAD, accounts for increased risk among diabetics compared with nondiabetics.
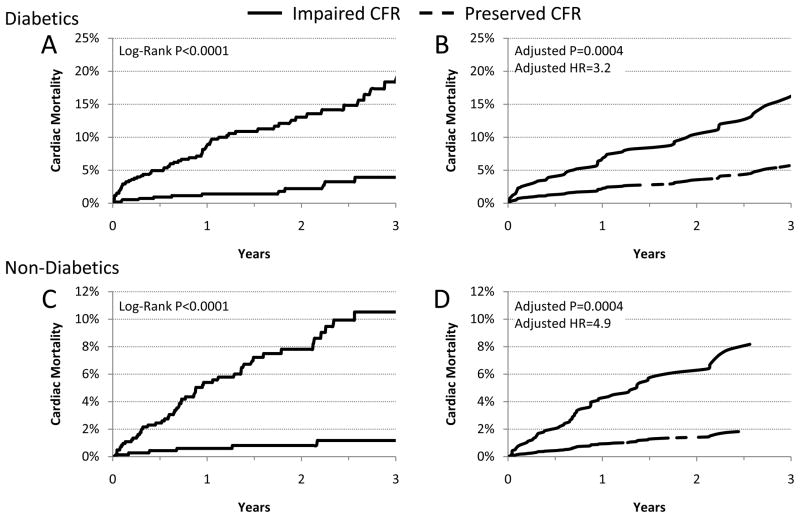
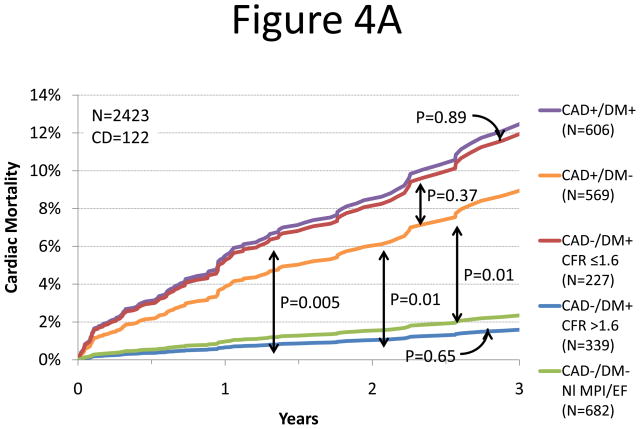
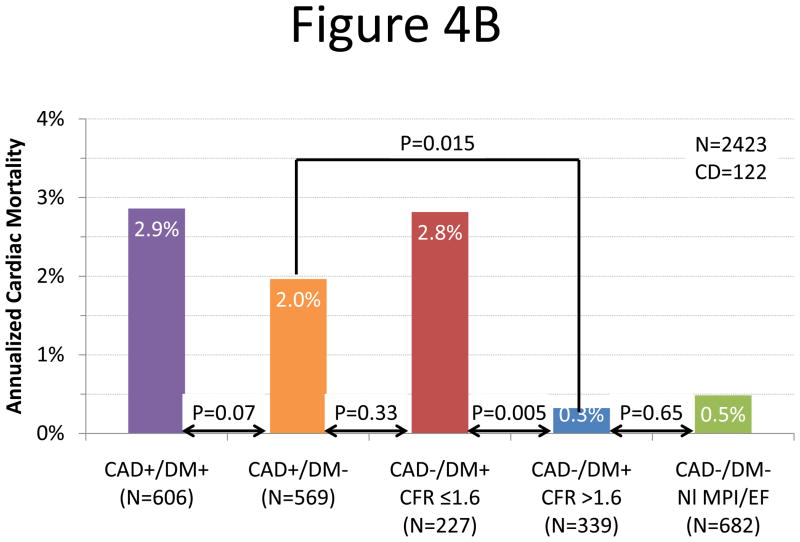
Methods and results: A total of 2783 consecutive patients (1172 diabetics and 1611 nondiabetics) underwent quantification of coronary flow reserve (CFR; CFR=stress divided by rest myocardial blood flow) by positron emission tomography and were followed up for a median of 1.4 years (quartile 1-3, 0.7-3.2 years). The primary end point was cardiac death. Impaired CFR (below the median) was associated with an adjusted 3.2- and 4.9-fold increase in the rate of cardiac death for diabetics and nondiabetics, respectively (P=0.0004). Addition of CFR to clinical and imaging risk models improved risk discrimination for both diabetics and nondiabetics (c index, 0.77-0.79, P=0.04; 0.82-0.85, P=0.03, respectively). Diabetic patients without known CAD with impaired CFR experienced a rate of cardiac death comparable to that for nondiabetic patients with known CAD (2.8%/y versus 2.0%/y; P=0.33). Conversely, diabetics without known CAD and preserved CFR had very low annualized cardiac mortality, which was similar to patients without known CAD or diabetes mellitus and normal stress perfusion and systolic function (0.3%/y versus 0.5%/y; P=0.65).
Conclusions: Coronary vasodilator dysfunction is a powerful, independent correlate of cardiac mortality among both diabetics and nondiabetics and provides meaningful incremental risk stratification. Among diabetic patients without CAD, those with impaired CFR have event rates comparable to those of patients with prior CAD, whereas those with preserved CFR have event rates comparable to those of nondiabetics.
Conflict of interest statement
Figures
Comment in
-
Enhanced risk stratification with noninvasive measurement of coronary flow reserve using positron emission tomography.Circulation. 2012 Oct 9;126(15):1808-11. doi: 10.1161/CIRCULATIONAHA.112.134569. Circulation. 2012. PMID: 23044605 No abstract available.
References
-
- Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, Mitch W, Smith SC, Sowers JR. Diabetes and Cardiovascular Disease: A Statement for Healthcare Professionals From the American Heart Association. Circulation. 1999;100:1134–1146. - PubMed
-
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285:2486–2497. - PubMed
-
- Giri S, Shaw LJ, Murthy DR, Travin MI, Miller DD, Hachamovitch R, Borges-Neto S, Berman DS, Waters DD, Heller GV. Impact of Diabetes on the Risk Stratification Using Stress Single-Photon Emission Computed Tomography Myocardial Perfusion Imaging in Patients With Symptoms Suggestive of Coronary Artery Disease. Circulation. 2002;105:32–40. - PubMed
-
- Rajagopalan N, Miller TD, Hodge DO, Frye RL, Gibbons RJ. Identifying high-risk asymptomatic diabetic patients who are candidates for screening stress single-photon emission computed tomography imaging. J Am Coll Cardiol. 2005;45:43–49. - PubMed
-
- Shaw L, Iskandrian A. Prognostic value of gated myocardial perfusion SPECT. J Nucl Cardiol. 2004;11:171–185. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
