Mesh complications in female pelvic floor reconstructive surgery and their management: A systematic review
- PMID: 22919127
- PMCID: PMC3424888
- DOI: 10.4103/0970-1591.98453
Mesh complications in female pelvic floor reconstructive surgery and their management: A systematic review
Abstract
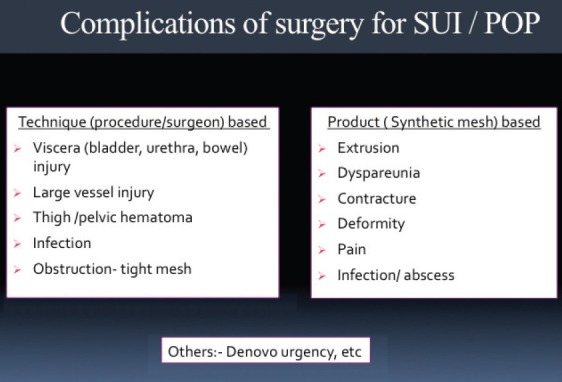
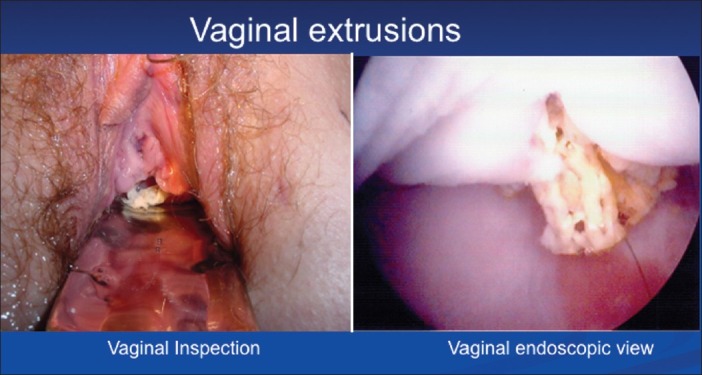
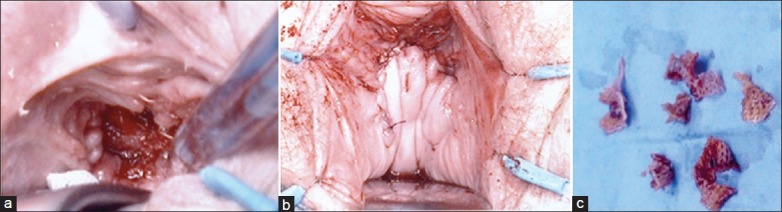
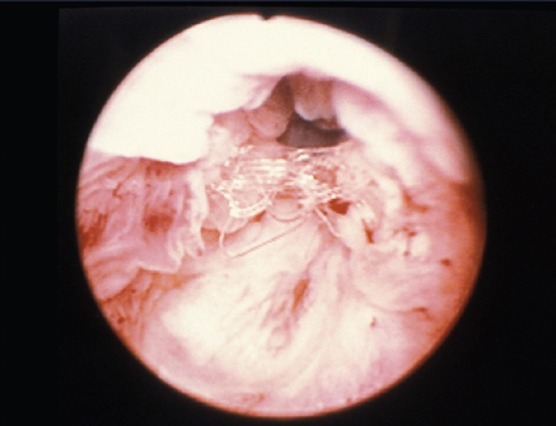
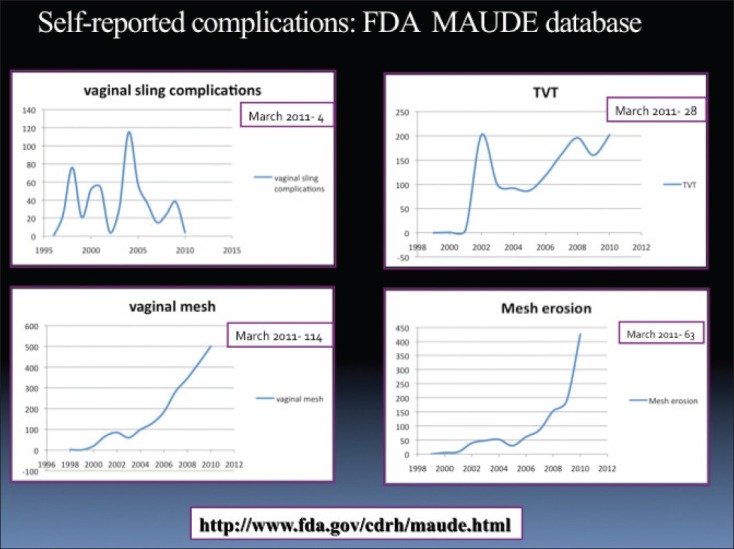
We reviewed the incidence, predisposing factors, presentation and management of complications related to the use of synthetic mesh in the management of stress urinary incontinence and pelvic organ prolapse repair. Immediate complications, such as bleeding, hematoma, injury to adjacent organs during placement of mesh and complication of voiding dysfunction are not discussed in this review, since they are primarily related to technique. A PubMed search of related articles published in English was done from April 2008 to March 2011. Key words used were urinary incontinence, mesh, complications, midurethral sling, anterior prolapse, anterior vaginal repair, pelvic organ prolapse, transvaginal mesh, vault prolapse, midurethral slings, female stress urinary incontinence, mesh erosion, vaginal mesh complications, and posterior vaginal wall prolapse. Since there were very few articles dealing with the management of mesh-related complications in the period covered in the search we extended the search from January 2005 onwards. Articles were selected to fit the scope of the topic. In addition, landmark publications and Manufacturer and User Facility Device Experience (MAUDE) data (FDA website) were included on the present topic. A total of 170 articles were identified. The use of synthetic mesh in sub-urethral sling procedures is now considered the standard for the surgical management of stress urinary incontinence. Synthetic mesh is being increasingly used in the management of pelvic organ prolapse. While the incidence of extrusion and erosion with mid-urethral sling is low, the extrusion rate in prolapse repair is somewhat higher and the use in posterior compartment remains controversial. When used through the abdominal approach the extrusion and erosion rates are lower. The management of mesh complication is an individualized approach. The choice of the technique should be based on the type of mesh complication, location of the extrusion and/or erosion, its magnitude, severity and potential recurrence of pelvic floor defect.
Keywords: Anterior vaginal repair; mesh complications; mid-urethral sling; pelvic organ prolapse; stress urinary incontinence.
Conflict of interest statement
Figures
References
-
- Nieminen K, Hiltunen R, Takala T, Heiskanen E, Merikari M, Niemi K, et al. Outcomes after anterior vaginal wall repair with mesh: A randomized, controlled trial with a 3 year follow-up. Am J Obstet Gynecol. 2010;203(235):e1–8. - PubMed
-
- Ignjatovic I, Stojkovic I, Basic D, Medojevic N, Potic M. Optimal primary minimally invasive treatment for patients with stress urinary incontinence and symptomatic pelvic organ prolapse: Tension free slings with colporrhaphy, or Prolift with the tension free midurethral sling? Eur J Obstet Gynecol Reprod Biol. 2010;50:97–101. - PubMed
-
- Nguyen JN, Burchette RJ. Outcome after anterior vaginal prolapse repair: A randomized controlled trial. Obstet Gynecol. 2008;111:891–8. - PubMed
-
- Withagen MI, Milani AL, den Boon J, Vervest HA, Vierhout ME. Trocar-guided mesh compared with conventional vaginal repair in recurrent prolapse: A randomized controlled trial. Obstet Gynecol. 2011;117(2 Pt 1):242–50. - PubMed
-
- Boreham MK, Wai CY, Miller RT, Schaffer JI, Word RA. Morphometric analysis of smooth muscle in the anterior vaginal wall of women with pelvic organ prolapse. Am J Obstet Gynecol. 2002;187:56–63. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous