

Impact of surgical volume on nationwide hospital mortality after pancreaticoduodenectomy
- PMID: 22919251
- PMCID: PMC3422799
- DOI: 10.3748/wjg.v18.i31.4175
Impact of surgical volume on nationwide hospital mortality after pancreaticoduodenectomy
Abstract
Aim: To evaluate the impact of surgical volume on nationwide hospital mortality after pancreaticoduodenectomy (PD) for periampullary tumors in South Korea.
Methods: Periampullary cancer patients who underwent PD between 2005 and 2008 were analyzed from the database of the Health Insurance Review and Assessment Service of South Korea. A total of 126 hospitals were divided into 5 categories, each similar in terms of surgical volume for each category. We used hospital mortality as a quality indicator, which was defined as death during the hospital stay for PD, and calculated adjusted mortality through multivariate logistic models using several confounder variables.
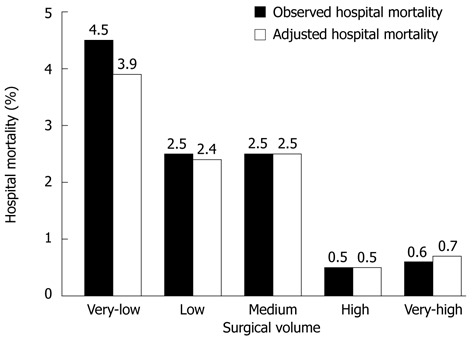
Results: A total of eligible 4975 patients were enrolled in this study. Average annual surgical volume of hospitals was markedly varied, ranging from 215 PDs in the very-high-volume hospital to < 10 PDs in the very-low-volume hospitals. Admission route, type of medical security, and type of operation were significantly different by surgical volume. The overall hospital mortality was 2.1% and the observed hospital mortality by surgical volume showed statistical difference. Surgical volume, age, and type of operation were independent risk factors for hospital death, and adjusted hospital mortality showed a similar difference between hospitals with observed mortality. The result of the Hosmer-Lemeshow test was 5.76 (P = 0.674), indicating an acceptable appropriateness of our regression model.
Conclusion: The higher-volume hospitals showed lower hospital mortality than the lower-volume hospitals after PD in South Korea, which were clarified through the nationwide database.
Keywords: Databases; Factual; Hospital mortality; Logistic models; Pancreaticoduodenectomy; Risk factors; South Korea.
Figures
Similar articles
-
Volume-outcome relationships in pancreatoduodenectomy for cancer.HPB (Oxford). 2016 Apr;18(4):317-24. doi: 10.1016/j.hpb.2016.01.515. Epub 2016 Feb 11. HPB (Oxford). 2016. PMID: 27037200 Free PMC article.
-
Temporal trends and volume-outcome associations in periampullary cancer patients: a propensity score-adjusted nationwide population-based study.Am J Surg. 2014 Apr;207(4):512-9. doi: 10.1016/j.amjsurg.2013.06.019. Epub 2013 Oct 26. Am J Surg. 2014. PMID: 24246262
-
Can we recommend surgical treatment to the octogenarian with periampullary cancer?: National database analysis in South Korea.Eur J Cancer. 2021 Feb;144:81-90. doi: 10.1016/j.ejca.2020.10.039. Epub 2020 Dec 17. Eur J Cancer. 2021. PMID: 33341449
-
Surgical Treatment of Ampullary Adenocarcinoma - Single Center Experience and a Review of Literature.Klin Onkol. 2017 Winter;31(1):46-52. doi: 10.14735/amko201846. Klin Onkol. 2017. PMID: 29488778 Review. English.
-
In-hospital survival after pancreatoduodenectomy is greater in high-volume hospitals versus lower-volume hospitals: a meta-analysis.ANZ J Surg. 2022 Jan;92(1-2):77-85. doi: 10.1111/ans.17293. Epub 2021 Oct 22. ANZ J Surg. 2022. PMID: 34676647
Cited by
-
Prospective minimally invasive pancreatic resections from the IGOMIPS registry: a snapshot of daily practice in Italy on 1191 between 2019 and 2022.Updates Surg. 2023 Sep;75(6):1439-1456. doi: 10.1007/s13304-023-01592-7. Epub 2023 Jul 20. Updates Surg. 2023. PMID: 37470915 Free PMC article.
-
Cancer care patterns in South Korea: Types of hospital where patients receive care and outcomes using national health insurance claims data.Cancer Med. 2023 Jul;12(13):14707-14717. doi: 10.1002/cam4.6093. Epub 2023 May 18. Cancer Med. 2023. PMID: 37199387 Free PMC article.
-
The 13-year experience of performing pancreaticoduodenectomy in a mid-volume municipal hospital.Ann Surg Treat Res. 2017 Feb;92(2):73-81. doi: 10.4174/astr.2017.92.2.73. Epub 2017 Jan 31. Ann Surg Treat Res. 2017. PMID: 28203554 Free PMC article.
-
Perioperative outcome after pancreatic head resection: a 10-year series of a specialized surgeon in a university hospital and a community hospital.J Gastrointest Surg. 2014 Aug;18(8):1434-40. doi: 10.1007/s11605-014-2555-8. Epub 2014 Jun 5. J Gastrointest Surg. 2014. PMID: 24898516
-
Pancreatoduodenectomy--current status of surgical and perioperative techniques in Germany.Langenbecks Arch Surg. 2013 Dec;398(8):1097-105. doi: 10.1007/s00423-013-1130-1. Epub 2013 Oct 19. Langenbecks Arch Surg. 2013. PMID: 24141987
References
-
- Afsari A, Zhandoug Z, Young S, Ferguson L, Silapaswan S, Mittal V. Outcome analysis of pancreaticoduodenectomy at a community hospital. Am Surg. 2002;68:281–284. - PubMed
-
- Schwartz GS, Swan RZ, Ruangvoravat L, Attiyeh FF. Morbidity and mortality after hepatic and pancreatic resections: results from one surgeon at a low-volume urban hospital over thirty years. Am J Surg. 2011;201:438–444. - PubMed
-
- Chew DK, Attiyeh FF. Experience with the Whipple procedure (pancreaticoduodenectomy) in a university-affiliated community hospital. Am J Surg. 1997;174:312–315. - PubMed
-
- Akhtar K, Perricone V, Chang D, Watson RJ. Experience of pancreaticoduodenectomy in a district general hospital. Br J Surg. 2000;87:362–373. - PubMed
-
- Topal B, Van de Sande S, Fieuws S, Penninckx F. Effect of centralization of pancreaticoduodenectomy on nationwide hospital mortality and length of stay. Br J Surg. 2007;94:1377–1381. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
