

Insulin resistance in patients with chronic kidney disease
- PMID: 22919275
- PMCID: PMC3420350
- DOI: 10.1155/2012/691369
Insulin resistance in patients with chronic kidney disease
Abstract
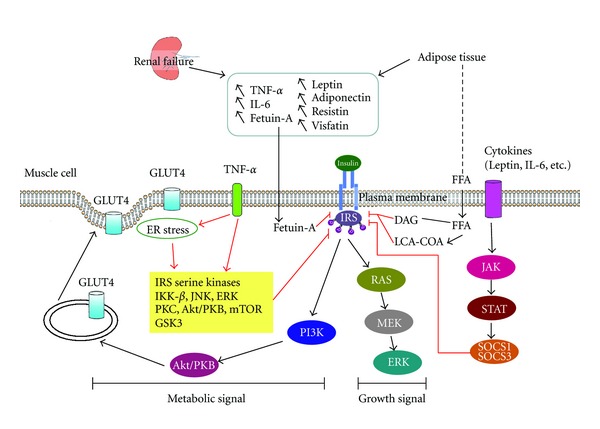
Metabolic syndrome and its components are associated with chronic kidney disease (CKD) development. Insulin resistance (IR) plays a central role in the metabolic syndrome and is associated with increased risk for CKD in nondiabetic patients. IR is common in patients with mild-to-moderate stage CKD, even when the glomerular filtration rate is within the normal range. IR, along with oxidative stress and inflammation, also promotes kidney disease. In patients with end stage renal disease, IR is an independent predictor of cardiovascular disease and is linked to protein energy wasting and malnutrition. Systemic inflammation, oxidative stress, elevated serum adipokines and fetuin-A, metabolic acidosis, vitamin D deficiency, depressed serum erythropoietin, endoplasmic reticulum stress, and suppressors of cytokine signaling all cause IR by suppressing insulin receptor-PI3K-Akt pathways in CKD. In addition to adequate renal replacement therapy and correction of uremia-associated factors, thiazolidinedione, ghrelin, protein restriction, and keto-acid supplementation are therapeutic options. Weight control, reduced daily prednisolone dosage, and the use of cyclosporin decrease the risk of developing new-onset diabetes after kidney transplantation. Improved understanding of the pathogenic mechanisms underlying IR in CKD may lead to more effective therapeutic strategies to reduce uremia-associated morbidity and mortality.
Figures
Similar articles
-
Relationship of insulin resistance to vitamin d status in children with nondiabetic chronic kidney disease.Saudi J Kidney Dis Transpl. 2017 Sep-Oct;28(5):1078-1084. doi: 10.4103/1319-2442.215144. Saudi J Kidney Dis Transpl. 2017. PMID: 28937066
-
Insulin resistance as a therapeutic target for chronic kidney disease.J Ren Nutr. 2015 Mar;25(2):226-9. doi: 10.1053/j.jrn.2014.10.019. Epub 2014 Dec 12. J Ren Nutr. 2015. PMID: 25511524 Review.
-
Hyperinsulinemia and insulin resistance, early cardiovascular risk factors in children with chronic kidney disease.Blood Purif. 2008;26(6):518-25. doi: 10.1159/000167799. Epub 2008 Nov 6. Blood Purif. 2008. PMID: 18987465
-
Insulin resistance as a predictor of cardiovascular morbidity and end-stage renal disease.J Diabetes Complications. 2015 Nov-Dec;29(8):1098-104. doi: 10.1016/j.jdiacomp.2015.05.010. Epub 2015 May 22. J Diabetes Complications. 2015. PMID: 26066409
-
Update on inflammation in chronic kidney disease.Blood Purif. 2015;39(1-3):84-92. doi: 10.1159/000368940. Epub 2015 Jan 20. Blood Purif. 2015. PMID: 25662331 Review.
Cited by
-
Ratio of C-Reactive Protein to Albumin Predicts Muscle Mass in Adult Patients Undergoing Hemodialysis.PLoS One. 2016 Oct 21;11(10):e0165403. doi: 10.1371/journal.pone.0165403. eCollection 2016. PLoS One. 2016. PMID: 27768746 Free PMC article.
-
Both insulin resistance and metabolic syndrome accelerate the progression of chronic kidney disease among Chinese adults: results from a 3-year follow-up study.Int Urol Nephrol. 2018 Dec;50(12):2239-2244. doi: 10.1007/s11255-018-1934-6. Epub 2018 Sep 4. Int Urol Nephrol. 2018. PMID: 30182294
-
Trends in insulin resistance: insights into mechanisms and therapeutic strategy.Signal Transduct Target Ther. 2022 Jul 6;7(1):216. doi: 10.1038/s41392-022-01073-0. Signal Transduct Target Ther. 2022. PMID: 35794109 Free PMC article. Review.
-
Association of NOS3 (rs 2070744) and SOD2Val16Ala (rs4880) gene polymorphisms with increased risk of ESRD among Egyptian patients.J Genet Eng Biotechnol. 2021 Oct 18;19(1):158. doi: 10.1186/s43141-021-00260-w. J Genet Eng Biotechnol. 2021. PMID: 34661767 Free PMC article.
-
Obesity and kidney disease: differential effects of obesity on adipose tissue and kidney inflammation and fibrosis.Curr Opin Nephrol Hypertens. 2015 Jan;24(1):28-36. doi: 10.1097/MNH.0000000000000087. Curr Opin Nephrol Hypertens. 2015. PMID: 25470014 Free PMC article. Review.
References
-
- Kasiske BL, Chavers B, Foley R, et al. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. American Journal of Kidney Diseases. 2002;39(2) supplement 1:S1–S266. - PubMed
-
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. American Journal of Kidney Diseases. 1998;32(5):S112–S119. - PubMed
-
- Muntner P, He J, Hamm L, Loria C, Whelton PK. Renal insufficiency and subsequent death resulting from cardiovascular disease in the United States. Journal of the American Society of Nephrology. 2002;13(3):745–753. - PubMed
-
- Grundy SM, Becker D, Clark LT, et al. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) Journal of the American Medical Association. 2001;285(19):2486–2497. - PubMed
-
- Kurella M, Lo JC, Chertow GM. Metabolic syndrome and the risk for chronic kidney disease among nondiabetic adults. Journal of the American Society of Nephrology. 2005;16(7):2134–2140. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical