Radiological features of metastatic gastrointestinal stromal tumors
- PMID: 22919557
- PMCID: PMC3424815
- DOI: 10.4103/2156-7514.99177
Radiological features of metastatic gastrointestinal stromal tumors
Abstract
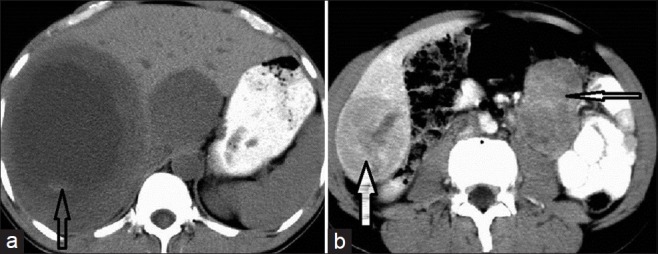
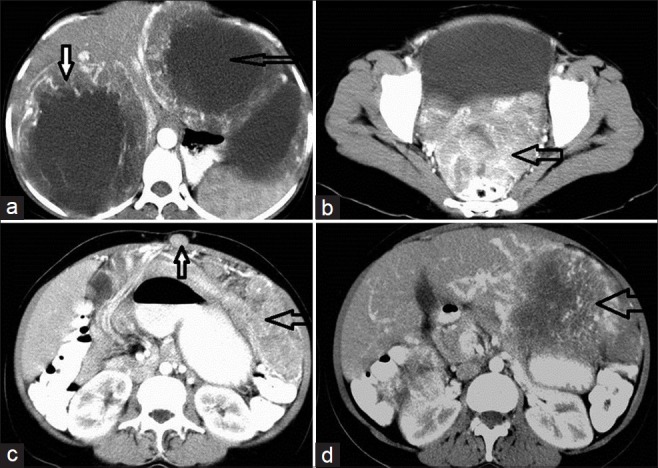
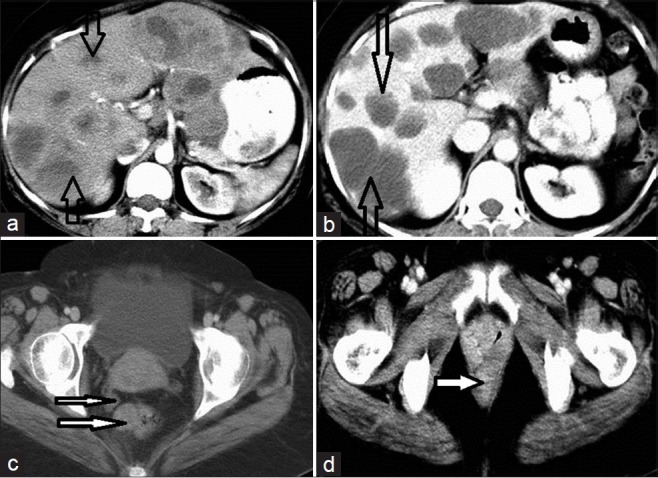
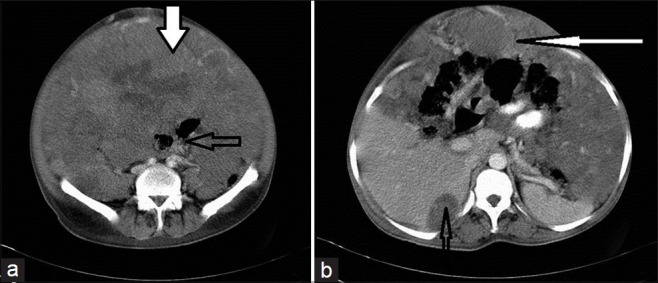
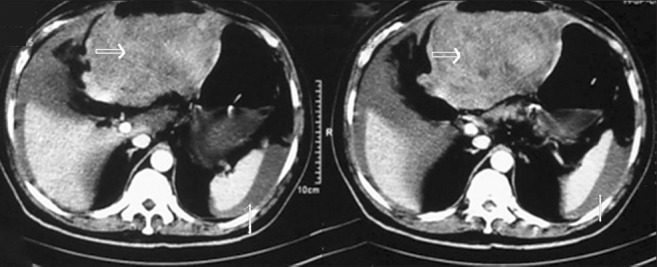
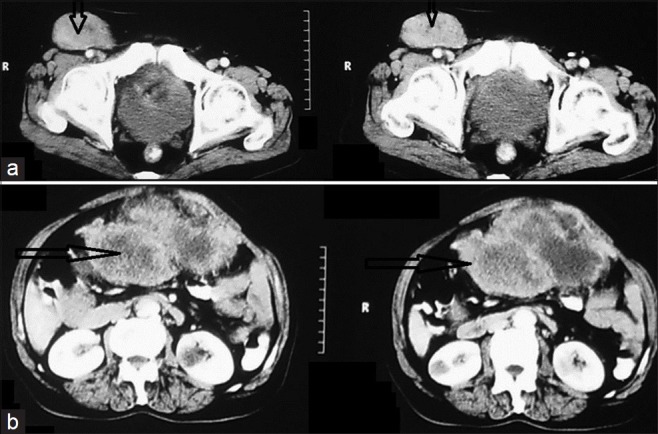
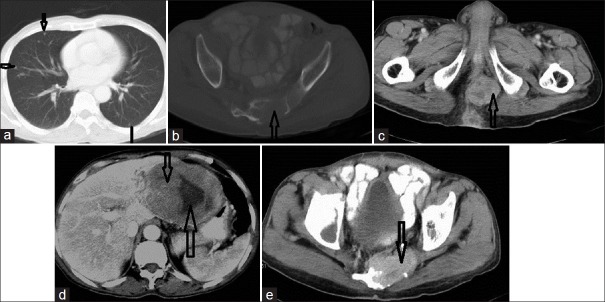
The imaging features of 42 histopathologically confirmed cases of Gastrointestinal Stromal Tumors (GIST) were analyzed, to observe the pattern of metastasis. At presentation 22 of 42 patients (52.3%) showed metastasis. During follow-up, three more cases developed metastasis, within one year of resection. Mesentery, omentum, and liver were the most frequent sites for metastasis. Other sites that were rarely reported to be involved were increasingly recognized to show metastasis due to longer survival. The metastasis often showed attenuation and enhancement characteristics, similar to primary GIST, and frequently showed necrosis, hemorrhage, and calcification.
Keywords: Gastrointestinal stromal tumor; gastrointestinal neoplasia; metastasis; sarcomas; smooth muscle mesenchymal tumor.
Conflict of interest statement
Figures



Similar articles
-
[Gastrointestinal stromal tumors (GIST) of the stomach as a cause of upper gastrointestinal bleeding].Acta Chir Iugosl. 2007;54(1):115-8. doi: 10.2298/aci0701115e. Acta Chir Iugosl. 2007. PMID: 17633870 Serbian.
-
[Clinicopathological and immunohistochemical study of extra-gastrointestinal stromal tumors arising from the omentum and mesentery].Zhonghua Bing Li Xue Za Zhi. 2005 Jan;34(1):11-4. Zhonghua Bing Li Xue Za Zhi. 2005. PMID: 15796875 Chinese.
-
Gastrointestinal stromal tumors/smooth muscle tumors (GISTs) primary in the omentum and mesentery: clinicopathologic and immunohistochemical study of 26 cases.Am J Surg Pathol. 1999 Sep;23(9):1109-18. doi: 10.1097/00000478-199909000-00015. Am J Surg Pathol. 1999. PMID: 10478672
-
Pathology and diagnostic criteria of gastrointestinal stromal tumors (GISTs): a review.Eur J Cancer. 2002 Sep;38 Suppl 5:S39-51. doi: 10.1016/s0959-8049(02)80602-5. Eur J Cancer. 2002. PMID: 12528772 Review.
-
Rare gastrointestinal stromal tumors (GIST): omentum and retroperitoneum.Transl Gastroenterol Hepatol. 2017 Dec 19;2:116. doi: 10.21037/tgh.2017.12.07. eCollection 2017. Transl Gastroenterol Hepatol. 2017. PMID: 29354773 Free PMC article. Review.
Cited by
-
Gastrointestinal Stromal Tumor (GIST) from esophagus to anorectum - diagnosis, response evaluation and surveillance on computed tomography (CT) scan.Indian J Radiol Imaging. 2019 Apr-Jun;29(2):133-140. doi: 10.4103/ijri.IJRI_354_18. Indian J Radiol Imaging. 2019. PMID: 31367084 Free PMC article.
-
Stereotactic ablative radiotherapy for bone metastasis of gastrointestinal stromal tumor: Case report and review of the literature.Rep Pract Oncol Radiother. 2020 May-Jun;25(3):331-335. doi: 10.1016/j.rpor.2020.02.013. Epub 2020 Feb 24. Rep Pract Oncol Radiother. 2020. PMID: 32256218 Free PMC article.
-
Gastrointestinal stromal tumor metastasis to the ovary: A case report.SAGE Open Med Case Rep. 2021 Apr 29;9:2050313X211012511. doi: 10.1177/2050313X211012511. eCollection 2021. SAGE Open Med Case Rep. 2021. PMID: 34017592 Free PMC article.
-
Gastrointestinal stromal tumours (GISTs): an insight into clinical practice with review of literature.Frontline Gastroenterol. 2017 Jan;8(1):19-25. doi: 10.1136/flgastro-2015-100670. Epub 2016 Jul 19. Frontline Gastroenterol. 2017. PMID: 28839880 Free PMC article.
-
Bacterial Involvement in Progression and Metastasis of Adenocarcinoma of the Stomach.Cancers (Basel). 2022 Oct 6;14(19):4886. doi: 10.3390/cancers14194886. Cancers (Basel). 2022. PMID: 36230809 Free PMC article. Review.
References
-
- Miettinen M, Lasota J. GIST - definition, clinical, histological, immunohistochemical and molecular-genetic features and differential diagnosis. Virchows Arch. 2001;438:1–12. - PubMed
-
- Daghter R, Cohen M, Williams G, Rothmann M, Gobburu J, Robbie G, et al. Imatinib mesylate in the treatment of metastatic and/or unresectable malignant gastrointestinal stromal tumours. Clin Cancer Res. 2002;8:3034–8. - PubMed
-
- Nilsson B, Bumming P, Meis-Kindblom JM, Oden A, Dortok A, Gustavsson B, et al. Gastrointestinal stromal tumors: The incidence, prevalence, clinical course and prognostication in pre-imatinib mesylate era: A population based study in western Sweden. Cancer. 2005;103:821–9. - PubMed
LinkOut - more resources
Full Text Sources