

Triggers and anatomical substrates in the genesis and perpetuation of atrial fibrillation
- PMID: 22920484
- PMCID: PMC3492815
- DOI: 10.2174/157340312803760721
Triggers and anatomical substrates in the genesis and perpetuation of atrial fibrillation
Abstract
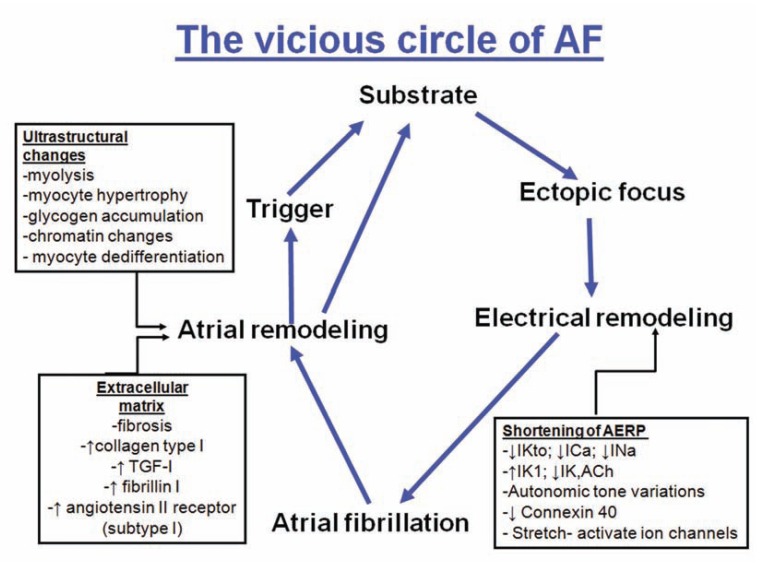
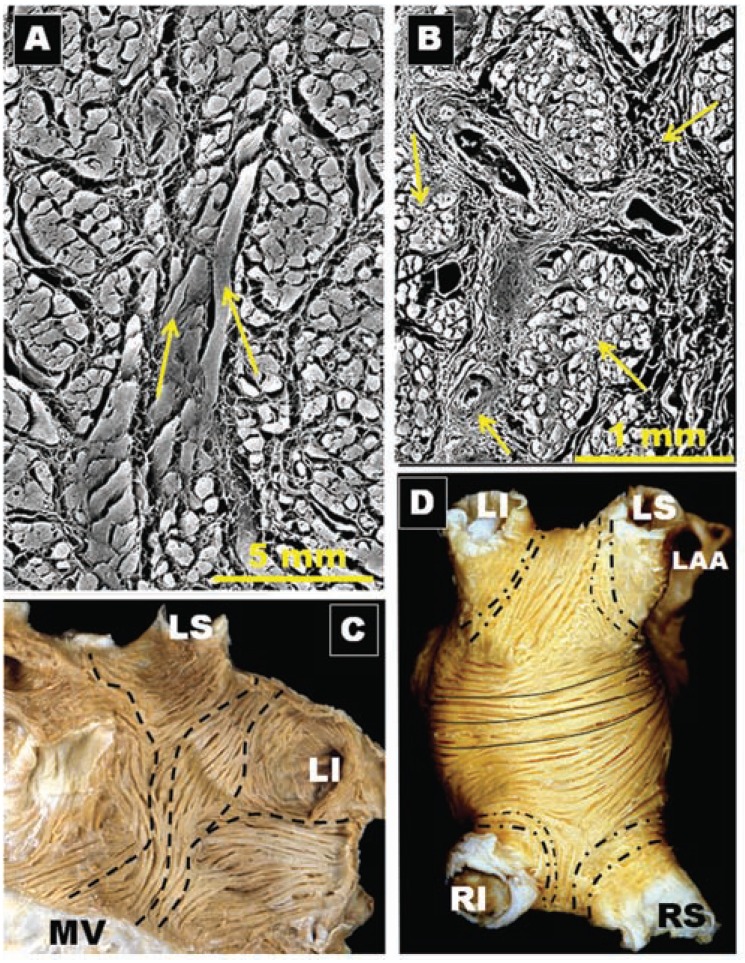
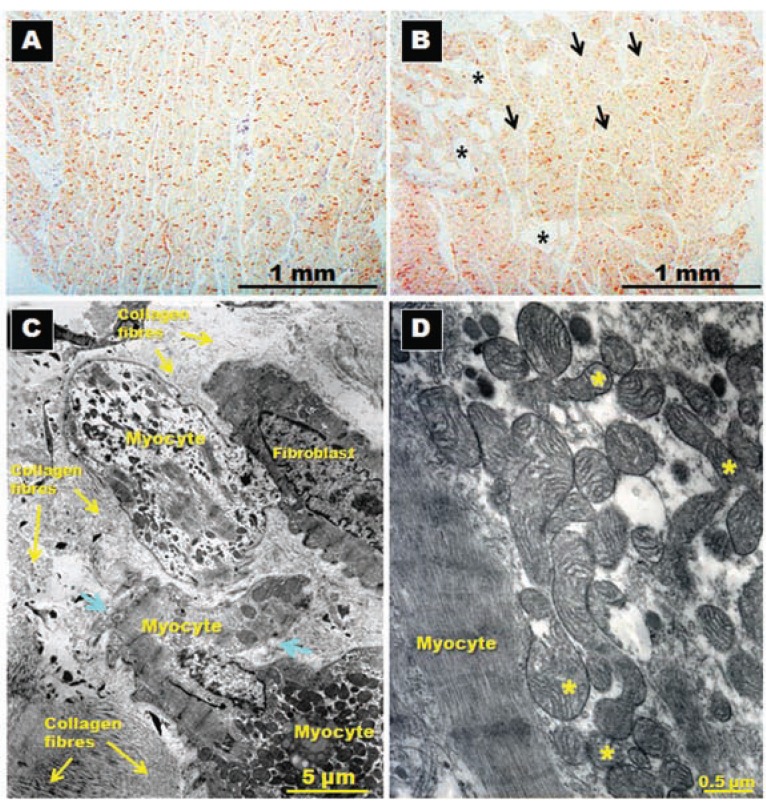
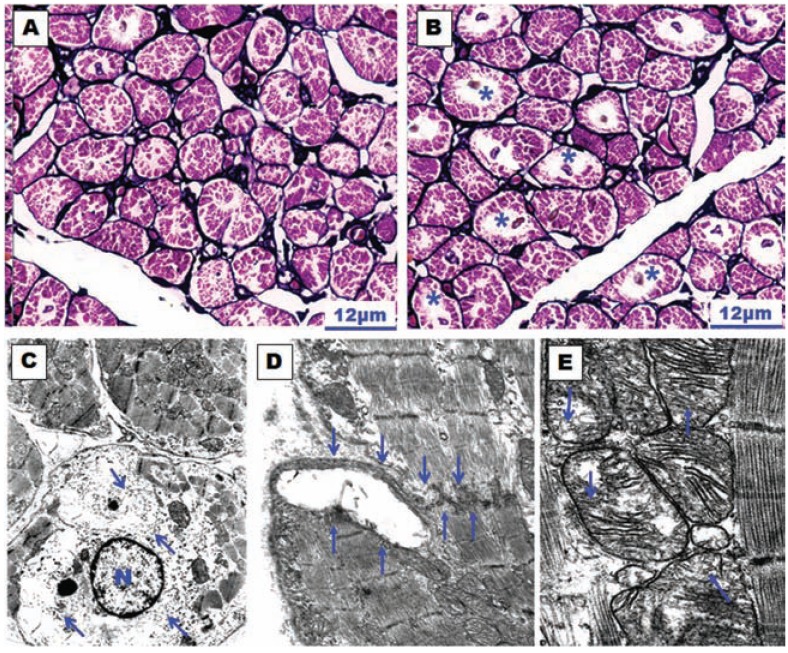
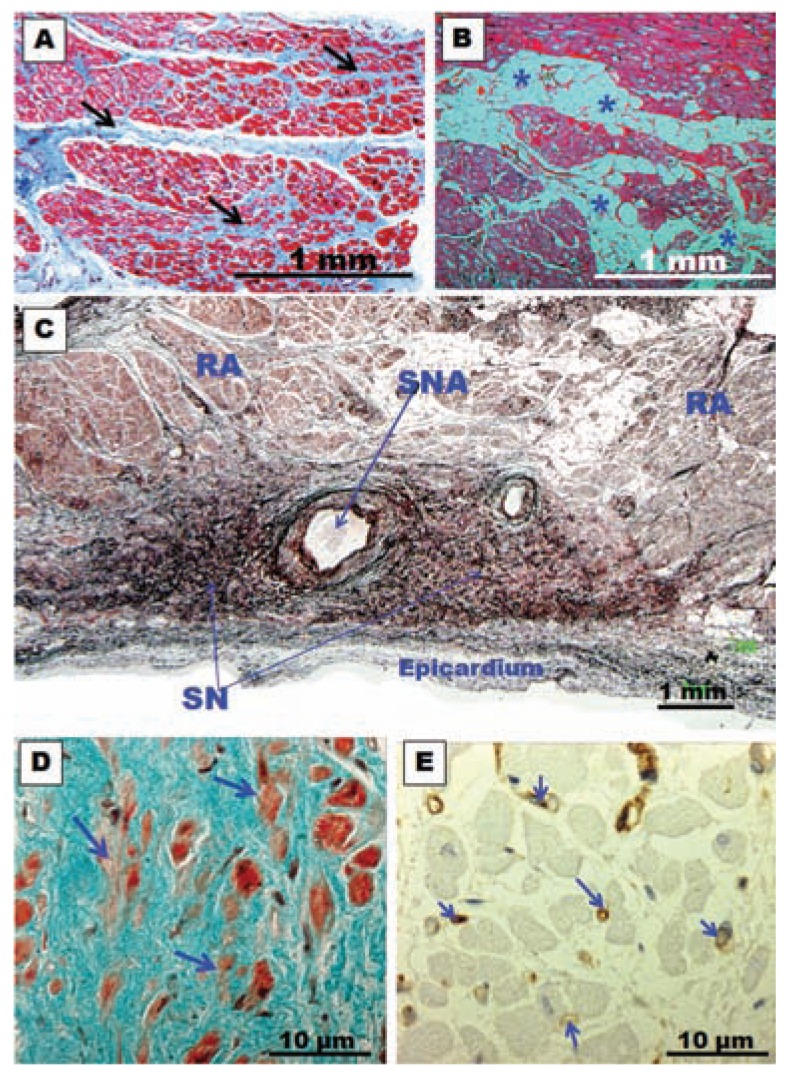
The definition of atrial fibrillation (AF) as a functional electrical disorder does not reflect the significant underlying structural abnormalities. Atrial and Pulmonary Vein (PV) muscle sleeve microstructural remodeling is present, and establishes a vulnerable substrate for AF maintenance. In spite of an incomplete understanding of the anatomo-functional basis for AF, current evidence demonstrates that this arrhythmia usually requires a trigger for initiation and a vulnerable electrophysiological and/or anatomical substrate for maintenance. It is still unclear whether the trigger mechanisms include focal enhanced automaticity, triggered activity and/or micro re-entry from myocardial tissue. Initiation of AF can be favored by both parasympathetic and sympathetic stimulation, which also seem to play a role in maintaining AF. Finally, evolving clinical evidence demonstrates that inflammation is associated with new-onset and recurrent AF through a mechanism that possibly involves cellular degeneration, apoptosis, and subsequent atrial fibrosis.
Figures
References
-
- Nattel S. New ideas about atrial fibrillation 50 years on. Nature. 2002;415(10 ):219–26. - PubMed
-
- Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10 ):659–66. - PubMed
-
- Hwang C, Wu TJ, Doshi RN, Peter CT, Chen PS. Vein of Marshall cannulation for the analysis of electrical activity in patients with focal atrial fibrillation. Circulation. 2000;101(13 ):1503–5. - PubMed
-
- Allessie MA, Bonke FI, Schopman FJ. Circus movement in rabbit atrial muscle as a mechanism of tachycardia. III. The leading circle concept: a new model of circus movement in cardiac tissue without the involvement of an anatomical obstacle. Circ Res. 1977;41(1 ):9–18. - PubMed
-
- Wijffels MC, Kirchhof CJ, Dorland R, et al. Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation. 1995;92(7 ):1954–68. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
