

Patient readmission and mortality after surgery for hepato-pancreato-biliary malignancies
- PMID: 22921328
- PMCID: PMC4051393
- DOI: 10.1016/j.jamcollsurg.2012.07.007
Patient readmission and mortality after surgery for hepato-pancreato-biliary malignancies
Abstract
Background: The incidence and associated risk factors for readmission after hepato-pancreato-biliary surgery are poorly characterized. The objective of the current study was to compare readmission after pancreatic vs hepatobiliary surgical procedures, as well as to identify potential factors associated with higher readmission within 30 days of discharge.
Study design: Using Surveillance, Epidemiology and End Results-Medicare linked data from 1986-2005, we identified 9,957 individuals aged 66 years and older who underwent complex hepatic, biliary, or pancreatic procedures for cancer treatment and were eligible for analysis. In-hospital morbidity, mortality, and 30-day readmission were examined.
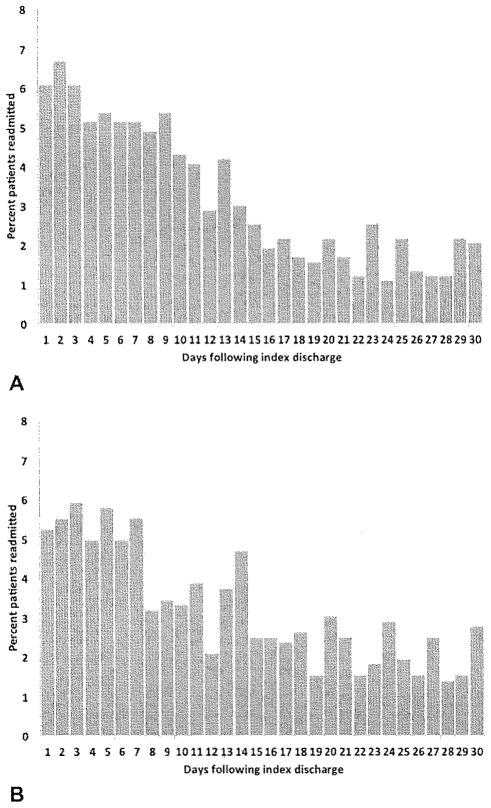
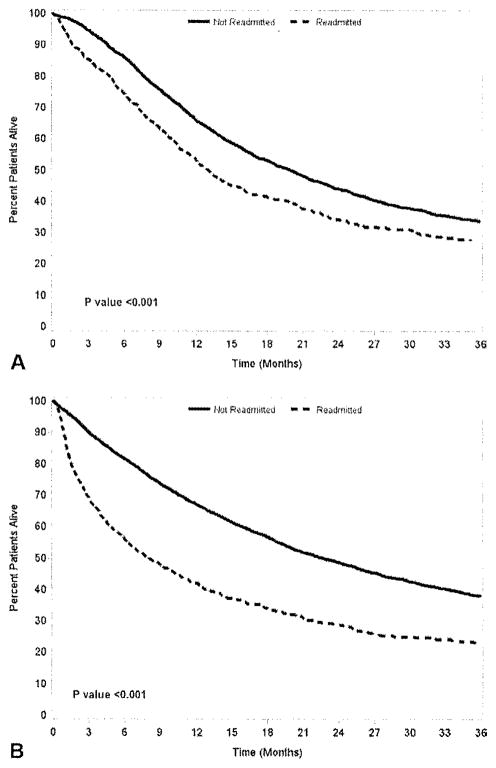
Results: Primary surgical treatment consisted of a pancreatic (46.7%), hepatic (50.0%), or biliary (3.4%) procedure. Mean patient age was 72.6 years and most patients were male (53.2%). The number of patients with multiple preoperative comorbidities increased over time (patients with Elixhauser's comorbidity score >13: 1986-1990, 47.0% vs 2001-2005, 62.9%; p < 0.001). Pancreatic operations had higher inpatient mortality vs hepatobiliary procedures (9.2% vs 7.3%; p < 0.001). Mean length of stay after pancreatic procedures was longer compared with hepatobiliary procedures (19.7 vs 10.3 days; p < 0.001). The proportion of patients readmitted after a pancreatic (1986-1990, 17.7%; 1991-1995, 16.1%; 1996-2000, 18.6%; 2001-2005, 19.6%; p = 0.15) or hepatobiliary (1986-1990, 14.3%; 1991-1995, 14.1%; 1996-2000, 15.2%; 2001-2005, 15.5%; p = 0.69) procedure did not change over time. Factors associated with increased risk of readmission included preoperative Elixhauser comorbidities >13 (odds ratio = 1.90) and prolonged index hospital stay ≥10 days (odds ratio = 1.54; both p < 0.05). During the readmission, additional morbidity and mortality were 46.5% and 8.0%, respectively.
Conclusions: Although the incidence of readmission did not change across the time periods examined, readmission was higher among patients undergoing a pancreatic procedure vs a hepatobiliary procedure. Other factors associated with risk of readmission included number of patient comorbidities and prolonged hospital stay. Readmission was associated with additional short-term morbidity and mortality.
Copyright © 2012 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Jencks SF. Defragmenting care. Ann Intern Med. 2010;153:757–758. - PubMed
-
- Martin RC, Brown R, Puffer L, et al. Readmission rates after abdominal surgery: the role of surgeon, primary caregiver, home health, and subacute rehab. Ann Surg. 2011;254:591–597. - PubMed
-
- van Bree SH, Vlug MS, Bemelman WA, et al. Faster recovery of gastrointestinal transit after laparoscopy and fast-track care in patients undergoing colonic surgery. Gastroenterology. 2011;141:872–880. e1–e4. - PubMed
-
- Kennedy EP, Rosato EL, Sauter PK, et al. Initiation of a critical pathway for pancreaticoduodenectomy at an academic institution—the first step in multidisciplinary team building. J Am Coll Surg. 2007;204:917–923. discussion 923–924. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
