

Dose of erythropoiesis-stimulating agents and adverse outcomes in CKD: a metaregression analysis
- PMID: 22921639
- PMCID: PMC3525813
- DOI: 10.1053/j.ajkd.2012.07.014
Dose of erythropoiesis-stimulating agents and adverse outcomes in CKD: a metaregression analysis
Abstract
Background: Targeting higher hemoglobin levels with erythropoiesis-stimulating agents (ESAs) to treat the anemia of chronic kidney disease (CKD) is associated with increased cardiovascular risk.
Study design: Metaregression analysis examining the association of ESA dose with adverse outcomes independent of target or achieved hemoglobin level.
Setting & population: Patients with anemia of CKD irrespective of dialysis status.
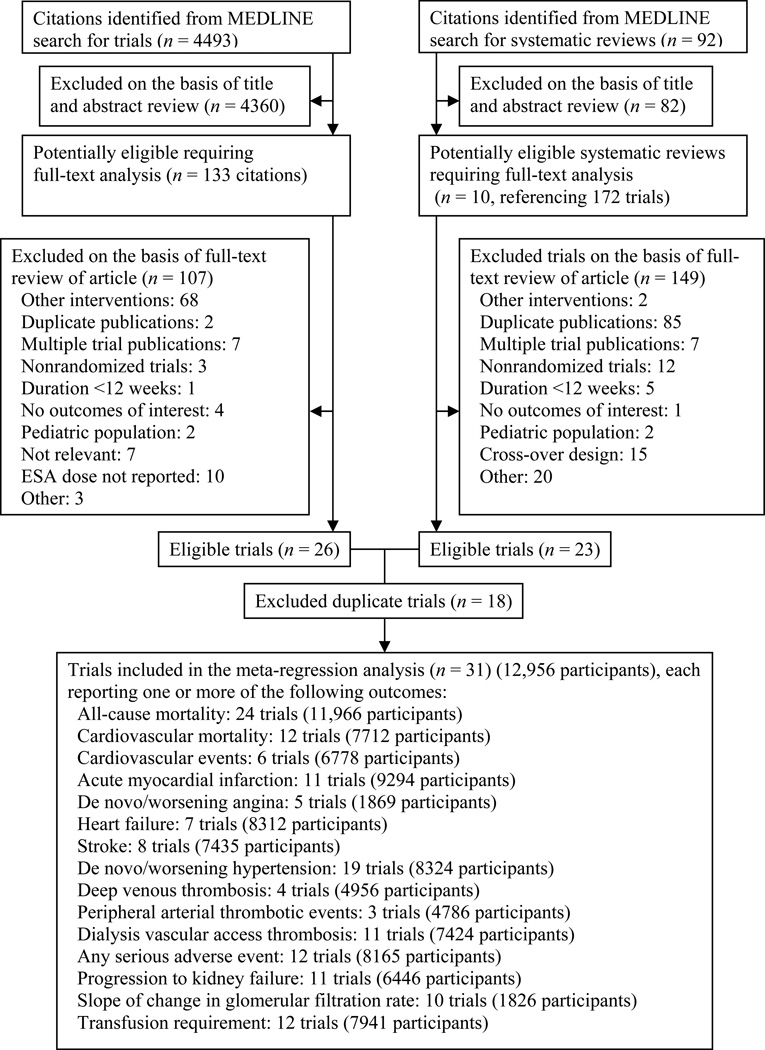
Selection criteria for studies: We searched MEDLINE (inception to August 2010) and bibliographies of published meta-analyses and selected randomized controlled trials assessing the efficacy of ESAs for the treatment of anemia in adults with CKD, with a minimum 3-month duration. Two authors independently screened citations and extracted relevant data. Individual study arms were treated as cohorts and constituted the unit of analysis.
Predictors: ESA dose standardized to a weekly epoetin alfa equivalent, and hemoglobin levels.
Outcomes: All-cause and cardiovascular mortality, cardiovascular events, kidney disease progression, or transfusion requirement.
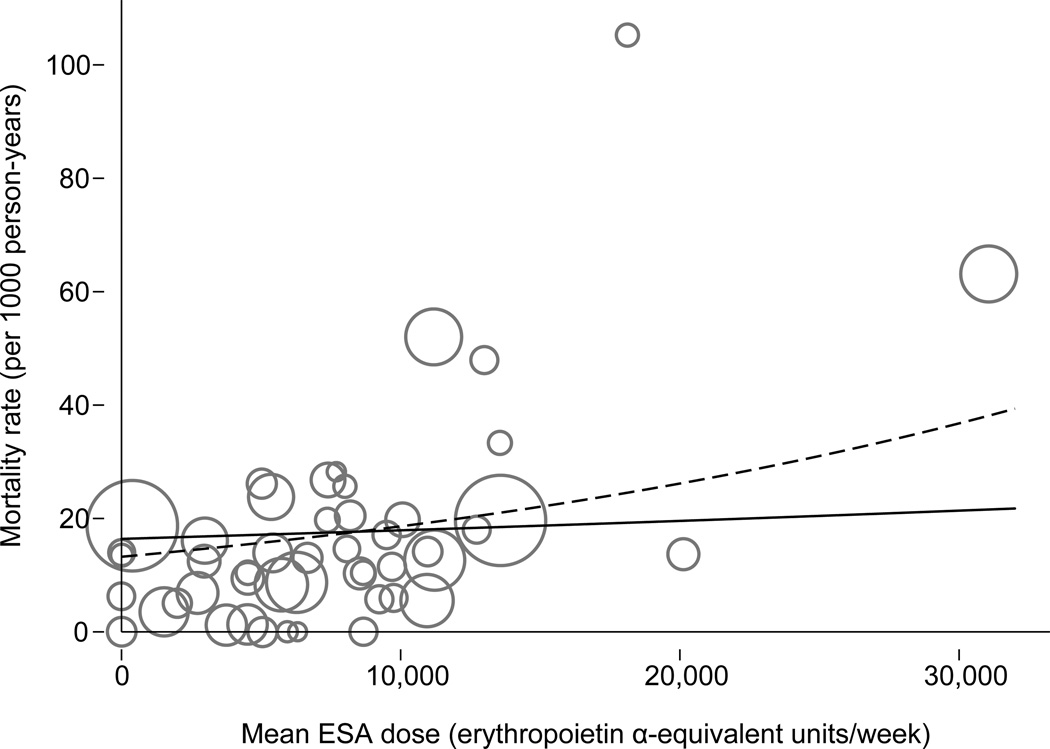
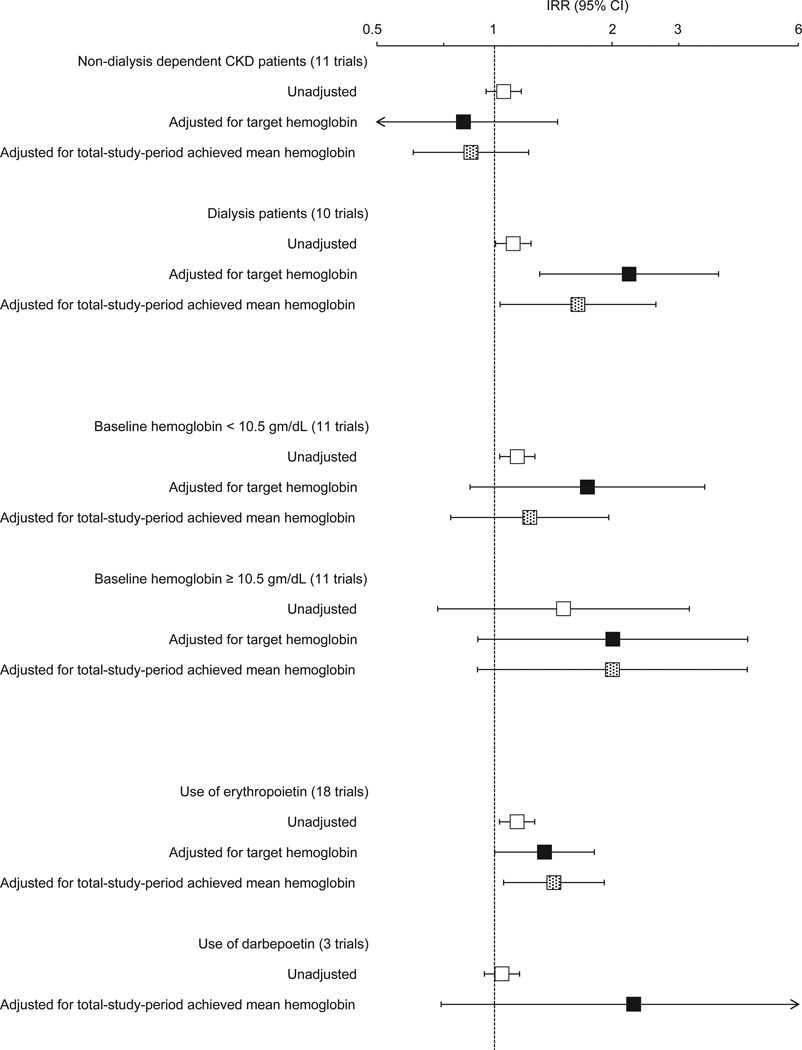
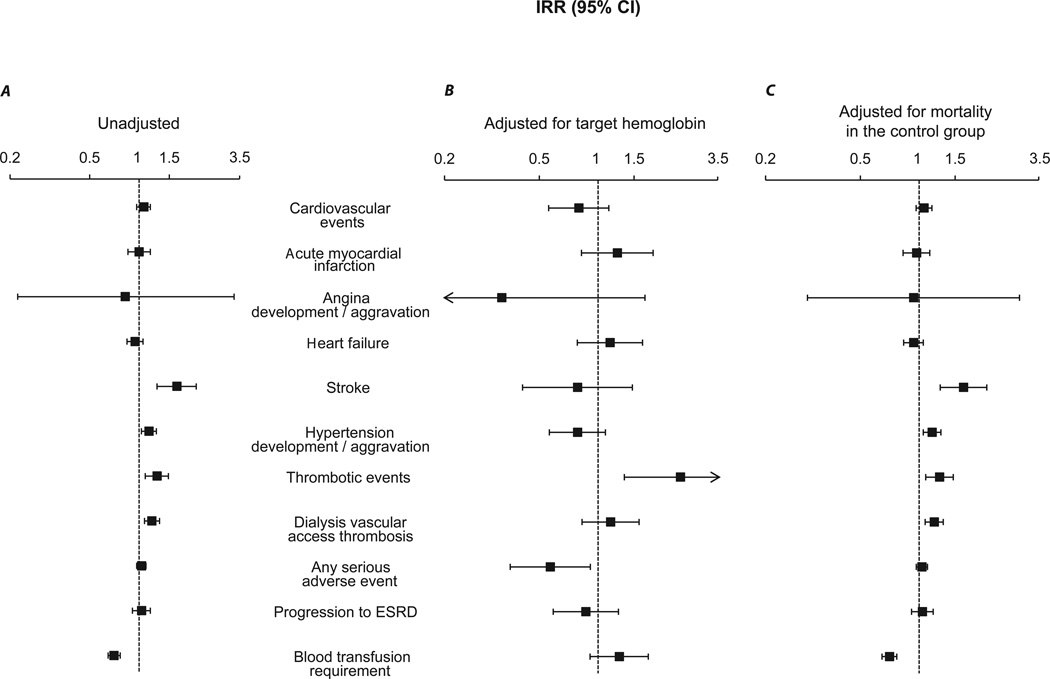
Results: 31 trials (12,956 patients) met the criteria. All-cause mortality was associated with higher (per epoetin alfa-equivalent 10,000-U/wk increment) first-3-month mean ESA dose (incidence rate ratio [IRR], 1.42; 95% CI, 1.10-1.83) and higher total-study-period mean ESA dose (IRR, 1.09; 95% CI, 1.02-1.18). First-3-month ESA dose remained significant after adjusting for first-3-month mean hemoglobin level (IRR, 1.48; 95% CI, 1.02-2.14), as did total-study-period mean ESA dose adjusting for target hemoglobin level (IRR, 1.41; 95% CI, 1.08-1.82). Parameter estimates between ESA dose and cardiovascular mortality were similar in magnitude and direction, but not statistically significant. Higher total-study-period mean ESA dose also was associated with increased rate of hypertension, stroke, and thrombotic events, including dialysis vascular access-related thrombotic events.
Limitations: Use of study-level aggregated data; use of epoetin alfa-equivalent doses; lack of adjustment for confounders.
Conclusions: In patients with CKD, higher ESA dose might be associated with all-cause mortality and cardiovascular complications independent of hemoglobin level.
Copyright © 2012 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Erythropoiesis-stimulating agents on trial: are higher dosages causing harm?Am J Kidney Dis. 2013 Jan;61(1):6-8. doi: 10.1053/j.ajkd.2012.10.004. Am J Kidney Dis. 2013. PMID: 23245737 No abstract available.
Similar articles
-
Effects of three kinds of erythropoiesis-stimulating agents on renal anemia in Japanese non-dialysis chronic kidney disease patients.Clin Exp Nephrol. 2014 Oct;18(5):755-62. doi: 10.1007/s10157-013-0919-0. Epub 2013 Dec 7. Clin Exp Nephrol. 2014. PMID: 24317507
-
Meta-analysis: erythropoiesis-stimulating agents in patients with chronic kidney disease.Ann Intern Med. 2010 Jul 6;153(1):23-33. doi: 10.7326/0003-4819-153-1-201007060-00252. Epub 2010 Jun 24. Ann Intern Med. 2010. PMID: 20439566 Review.
-
Daprodustat for the Treatment of Anemia in Patients Undergoing Dialysis.N Engl J Med. 2021 Dec 16;385(25):2325-2335. doi: 10.1056/NEJMoa2113379. Epub 2021 Nov 5. N Engl J Med. 2021. PMID: 34739194 Clinical Trial.
-
Renal prognoses by different target hemoglobin levels achieved by epoetin beta pegol dosing to chronic kidney disease patients with hyporesponsive anemia to erythropoiesis-stimulating agent: a multicenter open-label randomized controlled study.Clin Exp Nephrol. 2021 May;25(5):456-466. doi: 10.1007/s10157-020-02005-4. Epub 2021 Jan 7. Clin Exp Nephrol. 2021. PMID: 33411115 Clinical Trial.
-
Comparative efficacy and safety in ESA biosimilars vs. originators in adults with chronic kidney disease: a systematic review and meta-analysis.J Nephrol. 2018 Jun;31(3):321-332. doi: 10.1007/s40620-017-0419-5. Epub 2017 Jun 23. J Nephrol. 2018. PMID: 28646375
Cited by
-
The Relationship Between C-Reactive Protein (CRP) Concentrations and Erythropoietin Resistance, Hospital Admission Rate, Control of Mineral Metabolism, and Comorbidity in Hemodialysis Patients.Cureus. 2023 Nov 14;15(11):e48793. doi: 10.7759/cureus.48793. eCollection 2023 Nov. Cureus. 2023. PMID: 38098917 Free PMC article.
-
Biocompatibility of Surface-Modified Membranes for Chronic Hemodialysis Therapy.Biomedicines. 2022 Apr 3;10(4):844. doi: 10.3390/biomedicines10040844. Biomedicines. 2022. PMID: 35453594 Free PMC article. Review.
-
Use of erythropoiesis-stimulating agents in children with chronic kidney disease: a systematic review.Clin Kidney J. 2022 Feb 26;15(8):1483-1505. doi: 10.1093/ckj/sfac058. eCollection 2022 Aug. Clin Kidney J. 2022. PMID: 35892014 Free PMC article. Review.
-
Hemodialysis-induced cardiovascular disease.Semin Dial. 2018 May;31(3):258-267. doi: 10.1111/sdi.12694. Epub 2018 Apr 6. Semin Dial. 2018. PMID: 29624739 Free PMC article. Review.
-
Current Status of Renal Anemia Pharmacotherapy-What Can We Offer Today.J Clin Med. 2021 Sep 15;10(18):4149. doi: 10.3390/jcm10184149. J Clin Med. 2021. PMID: 34575261 Free PMC article. Review.
References
-
- Leaf DE, Goldfarb DS. Interpretation and review of health-related quality of life data in CKD patients receiving treatment for anemia. Kidney Int. 2009 Jan;75(1):15–24. - PubMed
-
- Jones M, Ibels L, Schenkel B, Zagari M. Impact of epoetin alfa on clinical end points in patients with chronic renal failure: a meta-analysis. Kidney Int. 2004 Mar;65(3):757–767. - PubMed
-
- Rao M, Pereira BJ. Optimal anemia management reduces cardiovascular morbidity, mortality, and costs in chronic kidney disease. Kidney Int. 2005 Oct;68(4):1432–1438. - PubMed
-
- Vlagopoulos PT, Tighiouart H, Weiner DE, et al. Anemia as a risk factor for cardiovascular disease and all-cause mortality in diabetes: the impact of chronic kidney disease. J Am Soc Nephrol. 2005 Nov;16(11):3403–3410. - PubMed
-
- Locatelli F, Pisoni RL, Combe C, et al. Anaemia in haemodialysis patients of five European countries: association with morbidity and mortality in the Dialysis Outcomes and Practice Patterns Study (DOPPS) Nephrol Dial Transplant. 2004 Jan;19(1):121–132. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
