

Obesity, prostate-specific antigen nadir, and biochemical recurrence after radical prostatectomy: biology or technique? Results from the SEARCH database
- PMID: 22921964
- PMCID: PMC3500618
- DOI: 10.1016/j.eururo.2012.08.015
Obesity, prostate-specific antigen nadir, and biochemical recurrence after radical prostatectomy: biology or technique? Results from the SEARCH database
Abstract
Background: Obesity is associated with an increased risk of biochemical recurrence (BCR) after radical prostatectomy (RP). It is unclear whether this is due to technical challenges related to operating on obese men or other biologic factors.
Objective: To examine whether obesity predicts higher prostate-specific antigen (PSA) nadir (as a measure of residual PSA-producing tissue) after RP and if this accounts for the greater BCR risk in obese men.
Design, setting, and participants: A retrospective analysis of 1038 RP patients from 2001 to 2010 in the multicenter US Veterans Administration-based Shared Equal Access Regional Cancer Hospital database with median follow-up of 41 mo.
Intervention: All patients underwent RP.
Outcome measurements and statistical analysis: We evaluated the relationship between body mass index (BMI) and ultrasensitive PSA nadir within 6 mo after RP. Adjusted proportional hazards models were used to examine the association between BMI and BCR with and without PSA nadir.
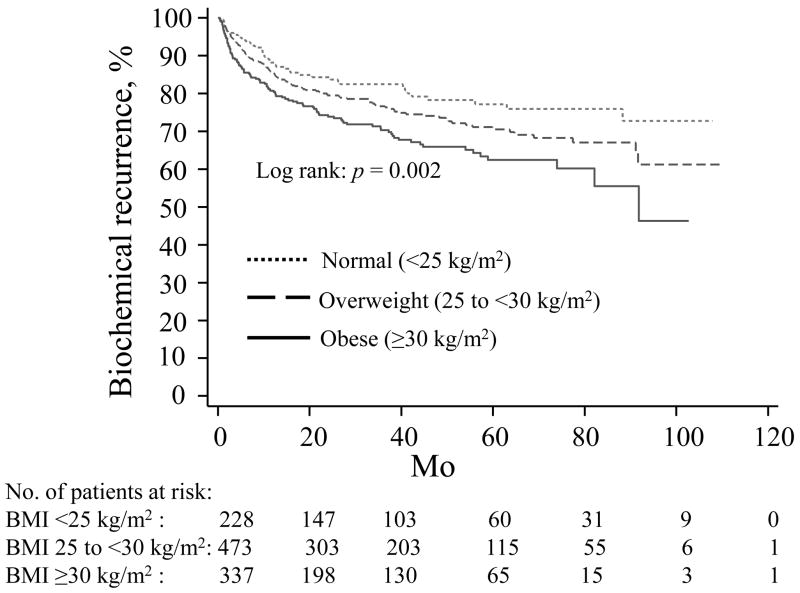
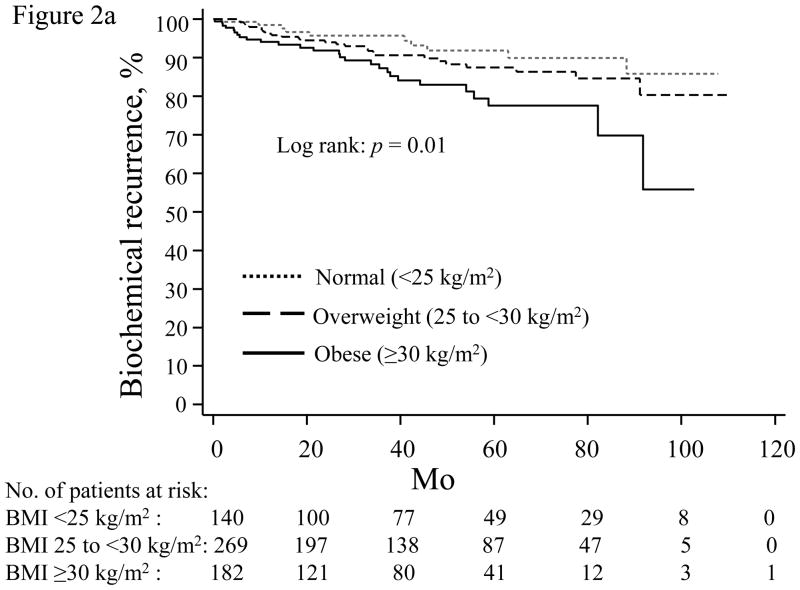
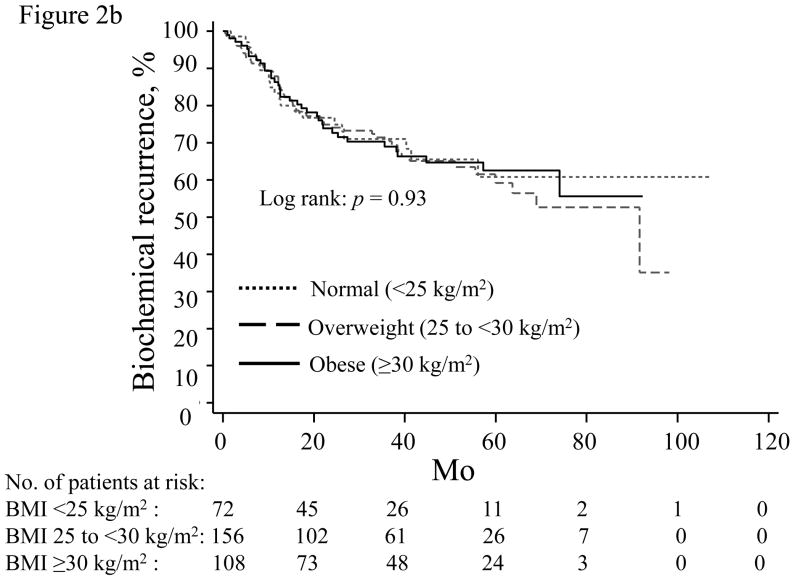
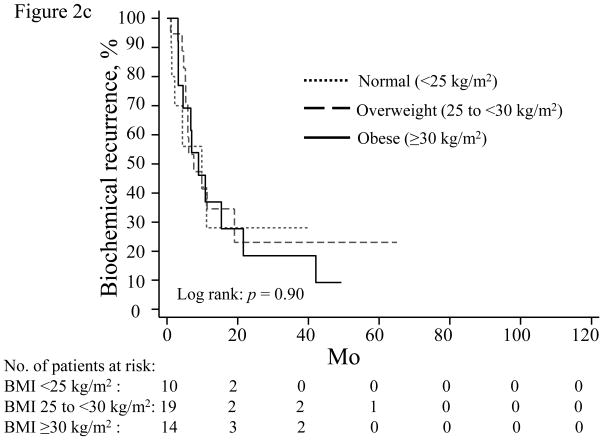
Results and limitations: Mean BMI was 28.5 kg/m2. Higher BMI was associated with higher PSA nadir on both univariable (p=0.001) and multivariable analyses (p<0.001). Increased BMI was associated with increased BCR risk (hazard ratio [HR]: 1.06; p=0.007). Adjusting for PSA nadir slightly attenuated, but did not eliminate, this association (HR: 1.04, p=0.043). When stratified by PSA nadir, obesity only significantly predicted BCR in men with an undetectable nadir (p=0.006). Unfortunately, other clinically relevant end points such as metastasis or mortality were not available.
Conclusions: Obese men are more likely to have a higher PSA nadir, suggesting that either more advanced disease or technical issues confound an ideal operation. However, even after adjusting for the increased PSA nadir, obesity remained predictive of BCR, suggesting that tumors in obese men are growing faster. This provides further support for the idea that obesity is biologically associated with prostate cancer progression.
Published by Elsevier B.V.
Figures
References
-
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999–2008. JAMA. 2010;303:235–41. - PubMed
-
- Global database on body mass index. [Accessed January 25, 2011.];World Health Organization. Web site http://apps.who.int/bmi/index.jsp.
-
- Laake I, Thune I, Selmer R, Tretli S, Slattery ML, Veierod MB. A prospective study of body mass index, weight change, and risk of cancer in the proximal and distal colon. Cancer Epidemiol Biomarkers Prev. 2010;19:1511–22. - PubMed
-
- Nomura AM. Body size and prostate cancer. Epidemiol Rev. 2001;23:126–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
