

Ectopic uterine tissue as a chronic pain generator
- PMID: 22922120
- PMCID: PMC3479308
- DOI: 10.1016/j.neuroscience.2012.08.033
Ectopic uterine tissue as a chronic pain generator
Abstract
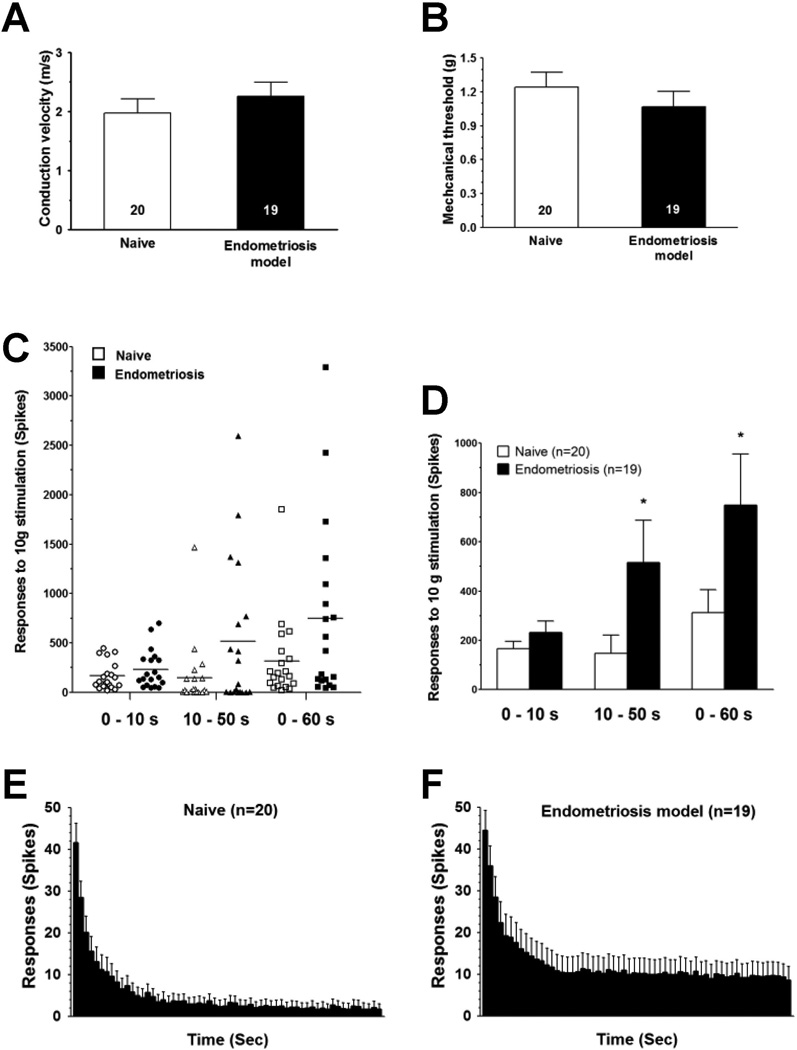
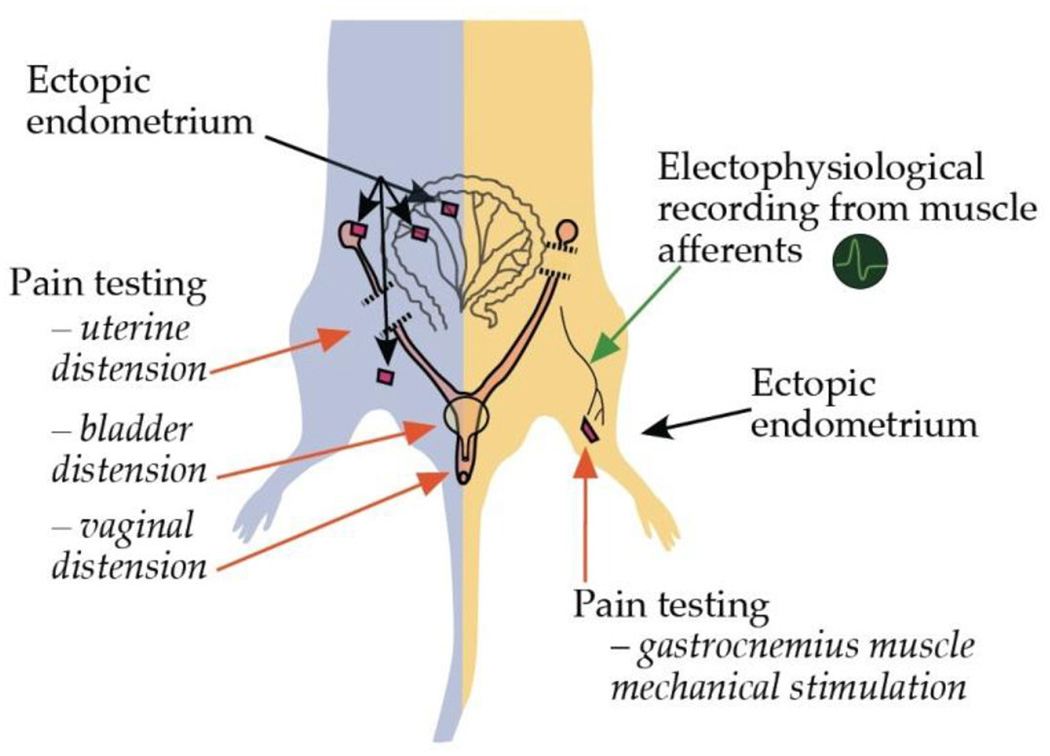
While chronic pain is a main symptom in endometriosis, the underlying mechanisms and effective therapy remain elusive. We developed an animal model enabling the exploration of ectopic endometrium as a source of endometriosis pain. Rats were surgically implanted with autologous uterus in the gastrocnemius muscle. Within two weeks, visual inspection revealed the presence of a reddish-brown fluid-filled cystic structure at the implant site. Histology demonstrated cystic glandular structures with stromal invasion of the muscle. Immunohistochemical studies of these lesions revealed the presence of markers for nociceptor nerve fibers and neuronal sprouting. Fourteen days after surgery rats exhibited persistent mechanical hyperalgesia at the site of the ectopic endometrial lesion. Intralesional, but not contralateral, injection of progesterone was dose-dependently antihyperalgesic. Systemic administration of leuprolide also produced antihyperalgesia. In vivo electrophysiological recordings from sensory neurons innervating the lesion revealed a significant increase in their response to sustained mechanical stimulation. These results are consistent with clinical and pathological findings observed in patients with endometriosis, compatible with the ectopic endometrium as a source of pain. This model of endometriosis allows mechanistic exploration at the lesion site facilitating our understanding of endometriosis pain.
Copyright © 2012 IBRO. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that no conflict of interest exists in connection with this study.
Figures





References
-
- Benowitz LI, Routtenberg A. GAP-43: an intrinsic determinant of neuronal development and plasticity. Trends Neurosci. 1997;20:84–91. - PubMed
-
- Berkley KJ, Cason A, Jacobs H, Bradshaw H, Wood E. Vaginal hyperalgesia in a rat model of endometriosis. Neurosci Lett. 2001;306:185–188. - PubMed
-
- Berkley KJ, Rapkin AJ, Papka RE. The pains of endometriosis. Science. 2005;308:1587–1589. - PubMed
-
- Botha AJ, Halliday AE, Flanagan JP. Endometriosis in gluteus muscle with surgical implantation. A case report. Acta Orthop Scand. 1991;62:497–499. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
