

Acute appendicitis in a duplicated appendix
- PMID: 22922359
- PMCID: PMC3437396
- DOI: 10.1016/j.ijscr.2012.08.004
Acute appendicitis in a duplicated appendix
Abstract
Introduction: Double appendix represents an extremely rare and commonly "missed" diagnosis, often with life threatening consequences.
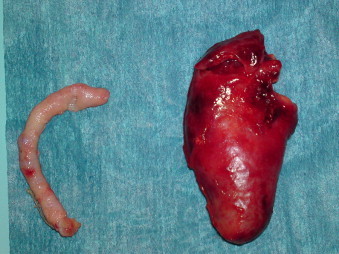
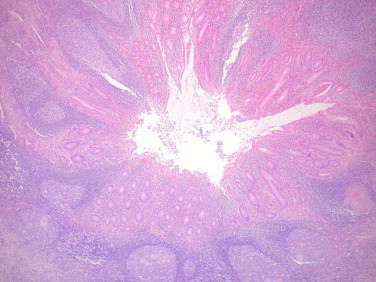
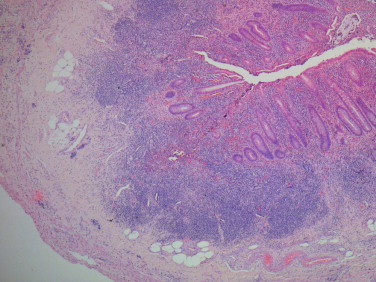
Presentation of case: In this case report we present an interesting case of operative treatment of acute appendicitis in a doubled vermiform appendix stemming operative pitfalls. A 23-year-old female was admitted to the emergency room department complaining of diffuse abdominal pain, nausea, and vomiting over the past 36h. As soon as the diagnosis of acute appendicitis was established a laparotomy via a McBurney incision was decided. Intraoperative findings included the presence of mild quantity of free fluid and surprisingly a thin non-inflamed appendiceal process. It was the preoperative ultrasound findings suggestive of acute appendicitis that dictated a more thorough investigation of the lower abdomen that led to the discovery of a second retrocecal inflamed appendix. Formal appendectomy was then performed for both processes. The patient had an uneventful recovery and was discharged on the fourth postoperative day.
Discussion: Double appendix represents a challenging clinical scenario in cases of right lower quadrant pain.
Conclusion: Life threatening consequences with legal extensions can arise from the incomplete removal of both stumps.
Copyright © 2012 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
Figures

References
-
- Collins D. A study of 50,000 specimens of the human vermiform appendix. Surgical Gynecological Obstetrics. 1955;101:437–446. - PubMed
-
- Kjossev K.T., Losanoff J.E. Duplicated vermiform appendix. British Journal of Surgery. 1996;83:1259. - PubMed
-
- Wallbridge P.H. Double appendix. British Journal of Surgery. 1963;50:346–347. - PubMed
-
- Mesko T.W., Lugo R., Breitholtz T. Horseshoe anomaly of the appendix: a previously undescribed entity. Surgery. 1989;106(3):563–566. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
