

Diagnostic accuracy of fractional flow reserve from anatomic CT angiography
- PMID: 22922562
- PMCID: PMC4281479
- DOI: 10.1001/2012.jama.11274
Diagnostic accuracy of fractional flow reserve from anatomic CT angiography
Abstract
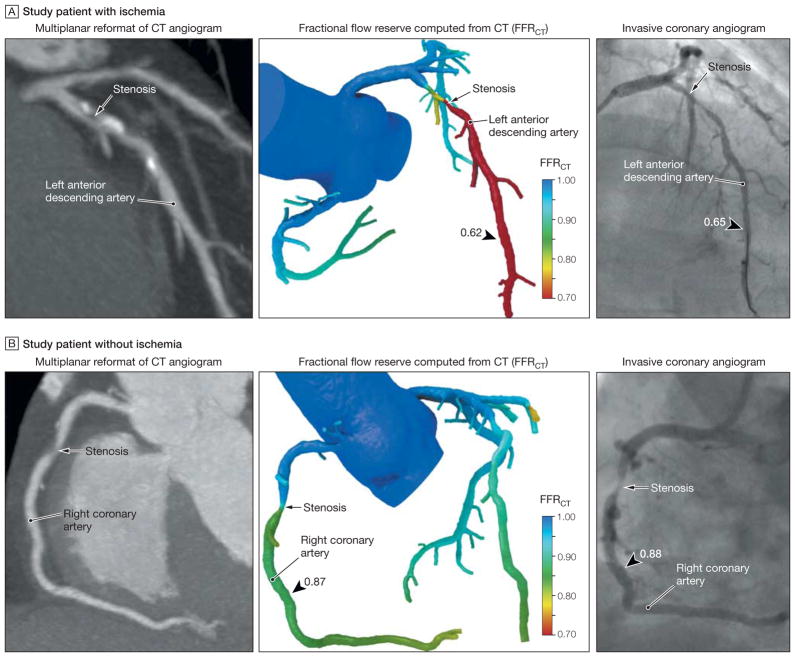
Context: Coronary computed tomographic (CT) angiography is a noninvasive anatomic test for diagnosis of coronary stenosis that does not determine whether a stenosis causes ischemia. In contrast, fractional flow reserve (FFR) is a physiologic measure of coronary stenosis expressing the amount of coronary flow still attainable despite the presence of a stenosis, but it requires an invasive procedure. Noninvasive FFR computed from CT (FFR(CT)) is a novel method for determining the physiologic significance of coronary artery disease (CAD), but its ability to identify ischemia has not been adequately examined to date.
Objective: To assess the diagnostic performance of FFR(CT) plus CT for diagnosis of hemodynamically significant coronary stenosis.
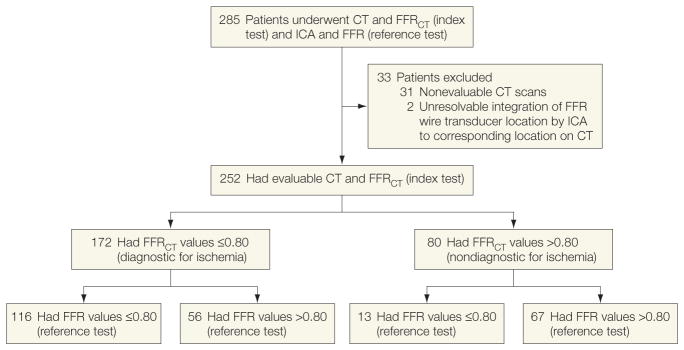
Design, setting, and patients: Multicenter diagnostic performance study involving 252 stable patients with suspected or known CAD from 17 centers in 5 countries who underwent CT, invasive coronary angiography (ICA), FFR, and FFR(CT) between October 2010 and October 2011. Computed tomography, ICA, FFR, and FFR(CT) were interpreted in blinded fashion by independent core laboratories. Accuracy of FFR(CT) plus CT for diagnosis of ischemia was compared with an invasive FFR reference standard. Ischemia was defined by an FFR or FFR(CT) of 0.80 or less, while anatomically obstructive CAD was defined by a stenosis of 50% or larger on CT and ICA.
Main outcome measures: The primary study outcome assessed whether FFR(CT) plus CT could improve the per-patient diagnostic accuracy such that the lower boundary of the 1-sided 95% confidence interval of this estimate exceeded 70%.
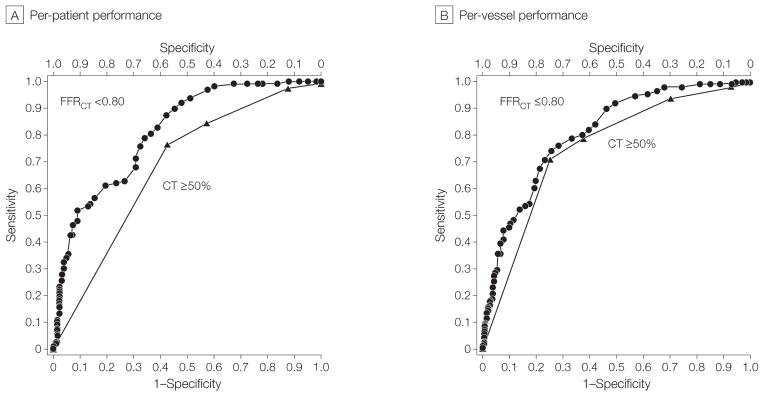
Results: Among study participants, 137 (54.4%) had an abnormal FFR determined by ICA. On a per-patient basis, diagnostic accuracy, sensitivity, specificity, positive predictive value, and negative predictive value of FFR(CT) plus CT were 73% (95% CI, 67%-78%), 90% (95% CI, 84%-95%), 54% (95% CI, 46%-83%), 67% (95% CI, 60%-74%), and 84% (95% CI, 74%-90%), respectively. Compared with obstructive CAD diagnosed by CT alone (area under the receiver operating characteristic curve [AUC], 0.68; 95% CI, 0.62-0.74), FFR(CT) was associated with improved discrimination (AUC, 0.81; 95% CI, 0.75-0.86; P < .001).
Conclusion: Although the study did not achieve its prespecified primary outcome goal for the level of per-patient diagnostic accuracy, use of noninvasive FFR(CT) plus CT among stable patients with suspected or known CAD was associated with improved diagnostic accuracy and discrimination vs CT alone for the diagnosis of hemodynamically significant CAD when FFR determined at the time of ICA was the reference standard.
Conflict of interest statement
Figures
Comment in
-
Detecting obstructive coronary disease with CT angiography and noninvasive fractional flow reserve.JAMA. 2012 Sep 26;308(12):1269-70. doi: 10.1001/2012.jama.11383. JAMA. 2012. PMID: 22922590 No abstract available.
-
Noninvasive approach to assess coronary artery stenoses and ischemia.JAMA. 2013 Jan 16;309(3):233-4. doi: 10.1001/jama.2012.157199. JAMA. 2013. PMID: 23321751 No abstract available.
-
Noninvasive approach to assess coronary artery stenoses and ischemia.JAMA. 2013 Jan 16;309(3):234. doi: 10.1001/jama.2012.157195. JAMA. 2013. PMID: 23321752 No abstract available.
-
Noninvasive approach to assess coronary artery stenoses and ischemia.JAMA. 2013 Jan 16;309(3):234-5. doi: 10.1001/jama.2012.157189. JAMA. 2013. PMID: 23321753 No abstract available.
-
Noninvasive approach to assess coronary artery stenoses and ischemia.JAMA. 2013 Jan 16;309(3):235-6. doi: 10.1001/jama.2012.157192. JAMA. 2013. PMID: 23321754 No abstract available.
-
Noninvasive approach to assess coronary artery stenoses and ischemia--reply.JAMA. 2013 Jan 16;309(3):236. doi: 10.1001/jama.2012.157208. JAMA. 2013. PMID: 23321755 No abstract available.
References
-
- Min JK, Shaw LJ, Berman DS. The present state of coronary computed tomography angiography a process in evolution. J Am Coll Cardiol. 2010;55(10):957–965. - PubMed
-
- Meijboom WB, Van Mieghem CA, van Pelt N, et al. Comprehensive assessment of coronary artery stenoses: computed tomography coronary angiography vs conventional coronary angiography and correlation with fractional flow reserve in patients with stable angina. J Am Coll Cardiol. 2008;52(8):636–643. - PubMed
-
- Schuijf JD, Bax JJ. CT angiography: an alternative to nuclear perfusion imaging? Heart. 2008;94(3):255–257. - PubMed
-
- Lauer MS. CT angiography: first things first. Circ Cardiovasc Imaging. 2009;2(1):1–3. - PubMed
-
- Hachamovitch R, Di Carli MF. Methods and limitations of assessing new noninvasive tests, I: anatomy-based validation of noninvasive testing. Circulation. 2008;117(20):2684–2690. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
