

The role of nutrition and body composition in peripheral arterial disease
- PMID: 22922595
- PMCID: PMC4535926
- DOI: 10.1038/nrcardio.2012.117
The role of nutrition and body composition in peripheral arterial disease
Abstract
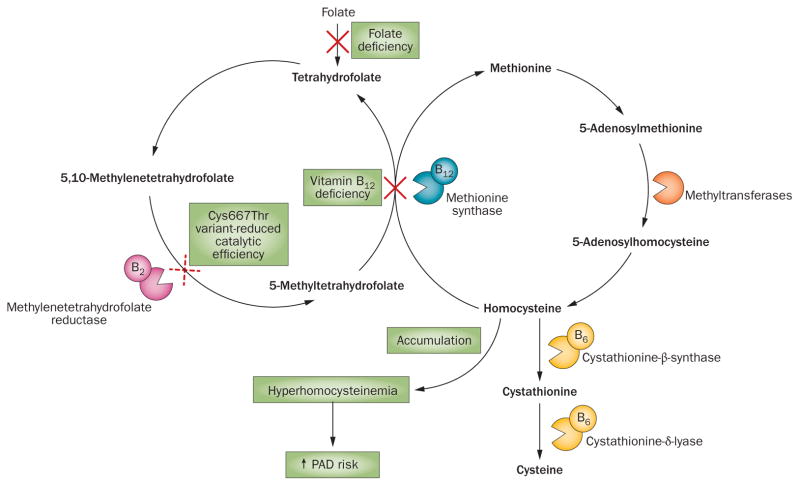
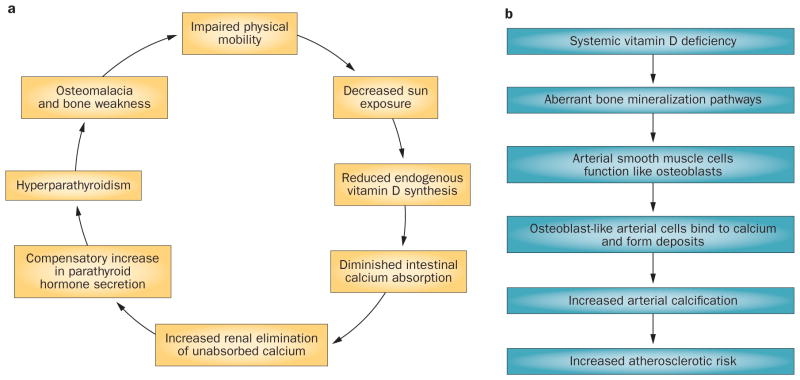
Peripheral arterial disease (PAD) has not been as extensively investigated as other cardiovascular diseases. However, the available data suggest that nutrition-based treatment strategies have the potential to reduce the cost-economic burden of PAD substantially. Abdominal obesity is associated with PAD and prospective and cross-sectional studies have shown that a low dietary intake of folate and reduced synthesis of vitamin D are associated with an increased risk of PAD and severe walking impairment in patients who have the disease. However, dietary patterns that are associated with decreased cardiovascular risk might protect against PAD. A small number of clinical trials have provided evidence that increased intakes of niacin and insoluble fiber might be associated with decreased levels of LDL cholesterol and thrombogenic biomarkers, as well as increased serum levels of HDL cholesterol in patients with PAD. However, little evidence that antioxidants, vitamins B(6) and B(12), or essential fatty acid supplements improve clinical outcomes in these patients exists. Overall, data on the effects of nutrition, body composition, and nutritional supplementation on the risk, progression, and prognosis of PAD are scarce. Further research into these areas is required to allow the development of evidence-based nutritional guidelines for the prevention and treatment of the disease.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Rice TW, Lumsden AB. Optimal medical management of peripheral arterial disease. Vasc Endovascular Surg. 2006;40:312–327. - PubMed
-
- Guidon M, McGee H. Exercise-based interventions and health-related quality of life in intermittent claudication: a 20-year (1989–2008) review. Eur J Cardiovasc Prev Rehabil. 2010;17:140–154. - PubMed
-
- Mahoney EM, et al. One-year costs in patients with a history of or at risk for atherothrombosis in the United States. Circ Cardiovasc Qual Outcomes. 2008;1:38–45. - PubMed
-
- Norgren L, et al. The next 10 years in the management of peripheral artery disease: perspectives from the ‘PAD 2009’ Conference. Eur J Vasc Endovasc Surg. 2010;40:375–380. - PubMed
-
- Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999–2000. Circulation. 2004;110:738–743. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
