

Trends in morbidity and mortality among very-low-birth-weight infants from 2003 to 2008 in Japan
- PMID: 22922774
- PMCID: PMC3547175
- DOI: 10.1038/pr.2012.114
Trends in morbidity and mortality among very-low-birth-weight infants from 2003 to 2008 in Japan
Abstract
Background: Although medical care for very-low-birth-weight (VLBW) infants has improved over time, it is unclear how this has affected mortality and morbidity. To characterize these trends, a network database was analyzed.
Methods: This is a cohort study of VLBW infants born from 2003 through 2008.
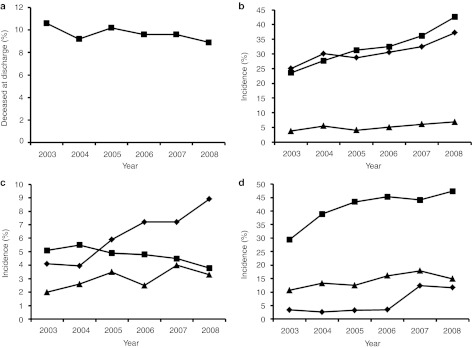
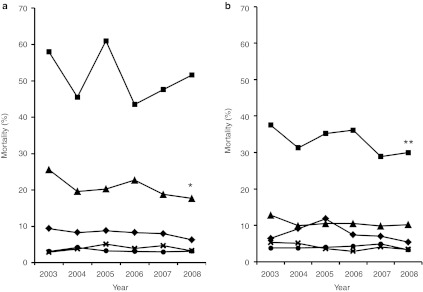
Results: Over the 6-y period, 19,344 infants were registered and analyzed. Crude mortality rates among the infants at discharge decreased significantly (from 10.8 to 8.7%) during the study period. The greatest improvement in mortality was observed among infants with birth weights between 501 and 750 g (25.6-17.7 %). The odds ratio (OR) of mortality over year adjusted for potential confounders by a logistic regression model was 0.94 (95% confidence interval 0.92-0.97). Significant increases were observed in some morbidities, including symptomatic patent ductus arteriosus with an OR of 1.11 (1.09-1.13); late-onset adrenal insufficiency, 1.21 (1.17-1.26); and necrotizing enterocolitis/intestinal perforation, 1.10 (1.01-1.12). However, the severe form of intraventricular hemorrhage, with an OR of 0.98 (0.92-0.99), decreased significantly. Risk-adjusted trends in other morbidities showed no significant change.
Conclusion: Mortality of VLBW infants decreased significantly over the 6-y study period. Decreasing morbidity is essential for further improvement in the outcomes in VLBW infants.
Figures
References
-
- Hack M, Horbar JD, Malloy MH, Tyson JE, Wright E, Wright L. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Network. Pediatrics. 1991;87:587–97. - PubMed
-
- Horbar JD, Badger GJ, Carpenter JH, Members of the Vermont Oxford Network et al. Trends in mortality and morbidity for very low birth weight infants, 1991–1999. Pediatrics. 2002;110 1 Pt 1:143–51. - PubMed
