

Posterior instrumentation, anterior column reconstruction with single posterior approach for treatment of pyogenic osteomyelitis of thoracic and lumbar spine
- PMID: 22922802
- PMCID: PMC3585646
- DOI: 10.1007/s00586-012-2487-5
Posterior instrumentation, anterior column reconstruction with single posterior approach for treatment of pyogenic osteomyelitis of thoracic and lumbar spine
Abstract
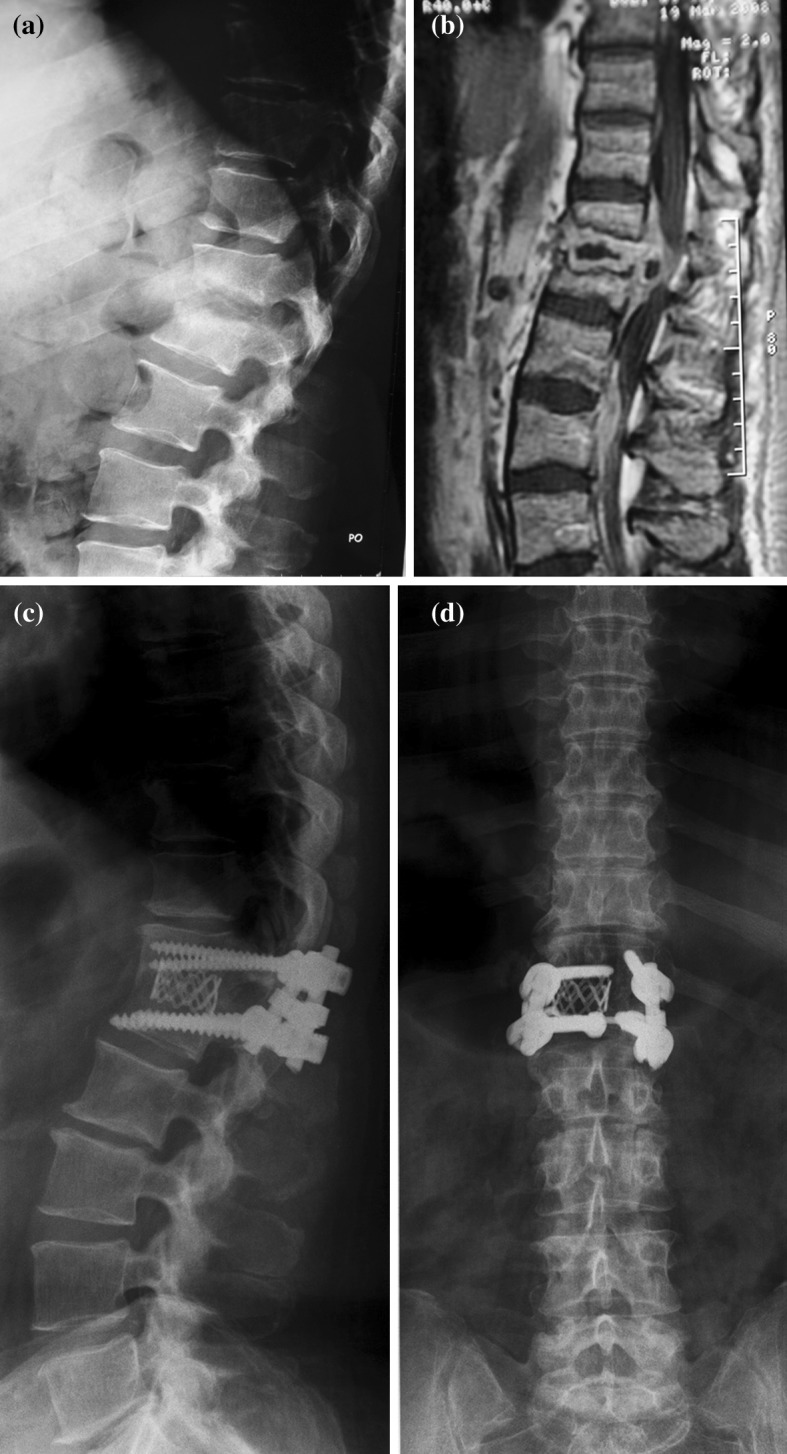
Purpose: Surgical treatment of thoracolumbar osteomyelitis consists of radical debridement, reconstruction of anterior column either with or without posterior stabilization. The objective of present study is to evaluate a case series of patients with osteomyelitis of thoracic and lumbar spine treated by single, posterior approach with posterior instrumentation and anterior column reconstruction.
Methods: Seventeen patients underwent clinical and radiological evaluation pre and postoperatively with latest follow-up at 19 months (8-56 months) after surgery. Parameters assessed were site of infection, causative organism, angle of deformity, blood loss, duration of surgery, ICU stay, deformity correction, time to solid bony fusion, ambulatory status, neurologic status (ASIA impairment scale), and functional outcome (Kirkaldy-Willis criteria).
Results: Mean operating time was 207 min and average blood loss 1,150 ml. Patients spent 2 (1-4) days in ICU and were able to walk unaided 1.6 (1-2) days after surgery. Infection receded in all 17 patients postoperatively. Solid bony fusion occurred in 15 out of 17 patients (88 %) on average 6.3 months after surgery. Functional outcome was assessed as excellent or good in 82 % of cases. Average deformity correction was 8 (1-18) degrees, with loss of correction of 4 (0-19) degrees at final follow-up.
Conclusions: Single, posterior approach addressing both columns poses safe alternative in treatment of pyogenic vertebral osteomyelitis of thoracic and lumbar spine. It proved to be less invasive resulting in faster postoperative recovery.
Figures


References
-
- Cramer J, Haase N, Behre I, Ostermann PAW. Spondylitis und spondylodiszitis. Trauma Berufskrankheit. 2003;5:336–341. doi: 10.1007/s10039-003-0771-7. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
