

Neuroinflammation, neuroautoimmunity, and the co-morbidities of complex regional pain syndrome
- PMID: 22923151
- PMCID: PMC3661922
- DOI: 10.1007/s11481-012-9392-x
Neuroinflammation, neuroautoimmunity, and the co-morbidities of complex regional pain syndrome
Abstract
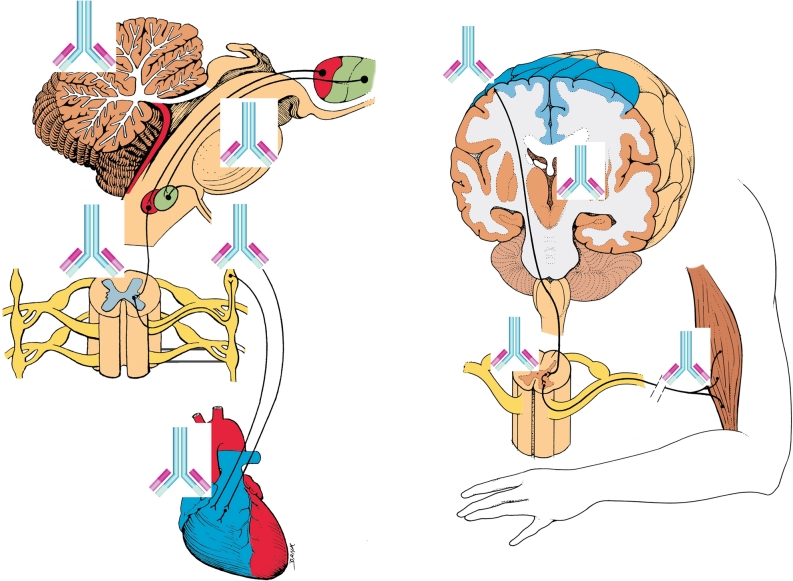
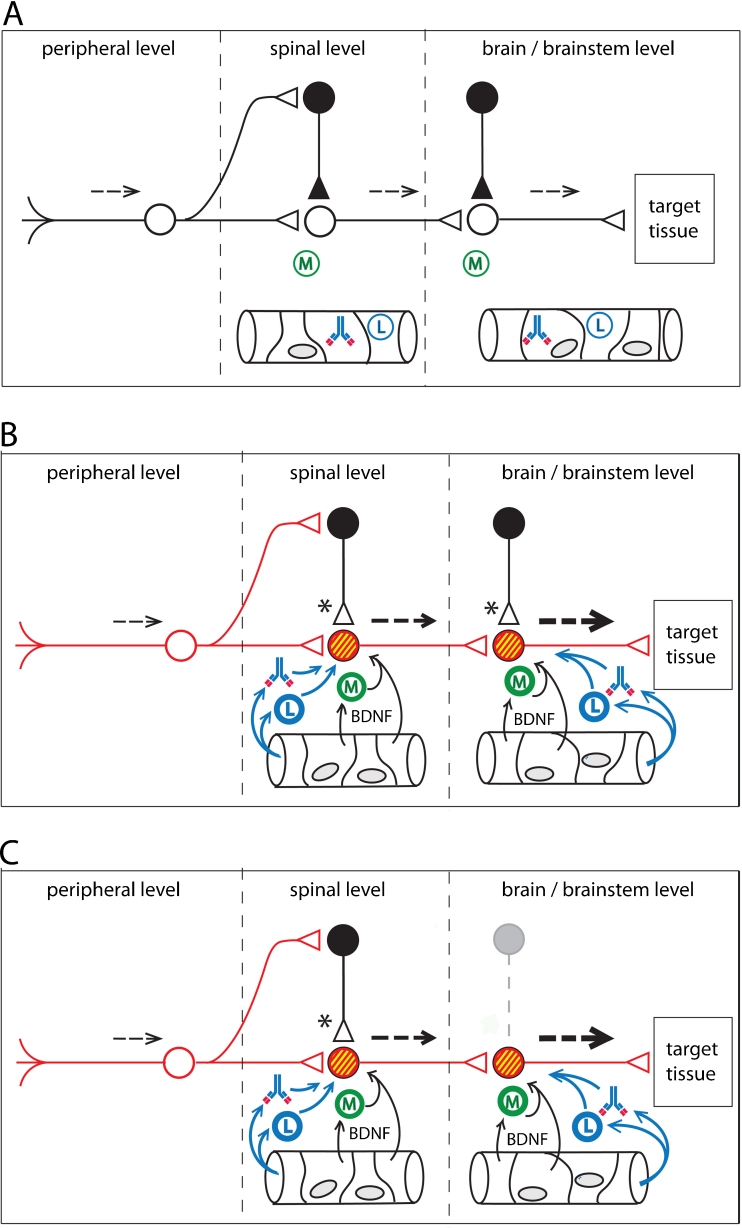
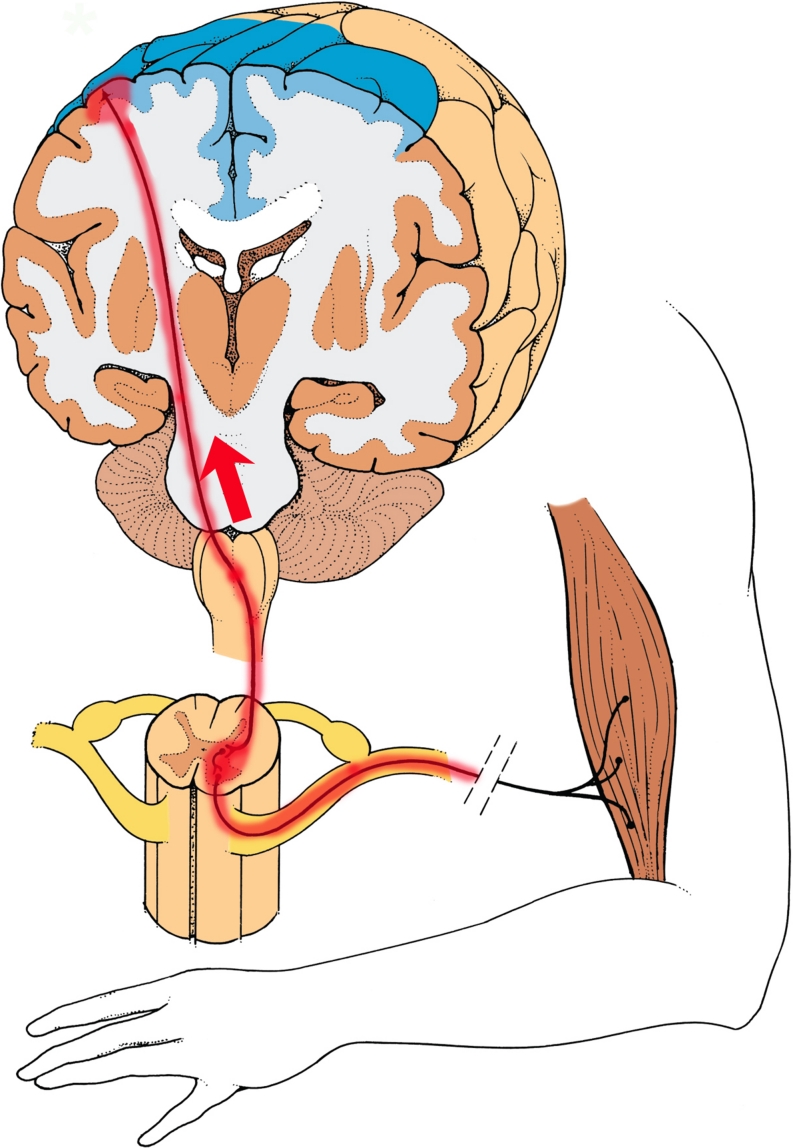
Complex Regional Pain Syndrome (CRPS) is associated with non-dermatomal patterns of pain, unusual movement disorders, and somatovisceral dysfunctions. These symptoms are viewed by some neurologists and psychiatrists as being psychogenic in origin. Recent evidence, however, suggests that an autoimmune attack on self-antigens found in the peripheral and central nervous system may underlie a number of CRPS symptoms. From both animal and human studies, evidence is accumulating that neuroinflammation can spread, either anterograde or retrograde, via axonal projections in the CNS, thereby establishing neuroinflammatory tracks and secondary neuroinflammatory foci within the neuraxis. These findings suggest that neuroinflammatory lesions, as well as their associated functional consequences, should be evaluated during the differential diagnosis of non-dermatomal pain presentations, atypical movement disorders, as well as other "medically unexplained symptoms", which are often attributed to psychogenic illness.
Figures
References
-
- Alafaci C, Salpietro FM, Montemagno G, Grasso G, Tomasello F. Spasmodic torticollis due to neurovascular compression of the spinal accessory nerve by the anteroinferior cerebellar artery: Case report. Neurosurgery. 2000;47:768–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
