

Near-Infrared Fluorescence Imaging in Humans with Indocyanine Green: A Review and Update
- PMID: 22924087
- PMCID: PMC3424734
- DOI: 10.2174/1876504101002010012
Near-Infrared Fluorescence Imaging in Humans with Indocyanine Green: A Review and Update
Abstract
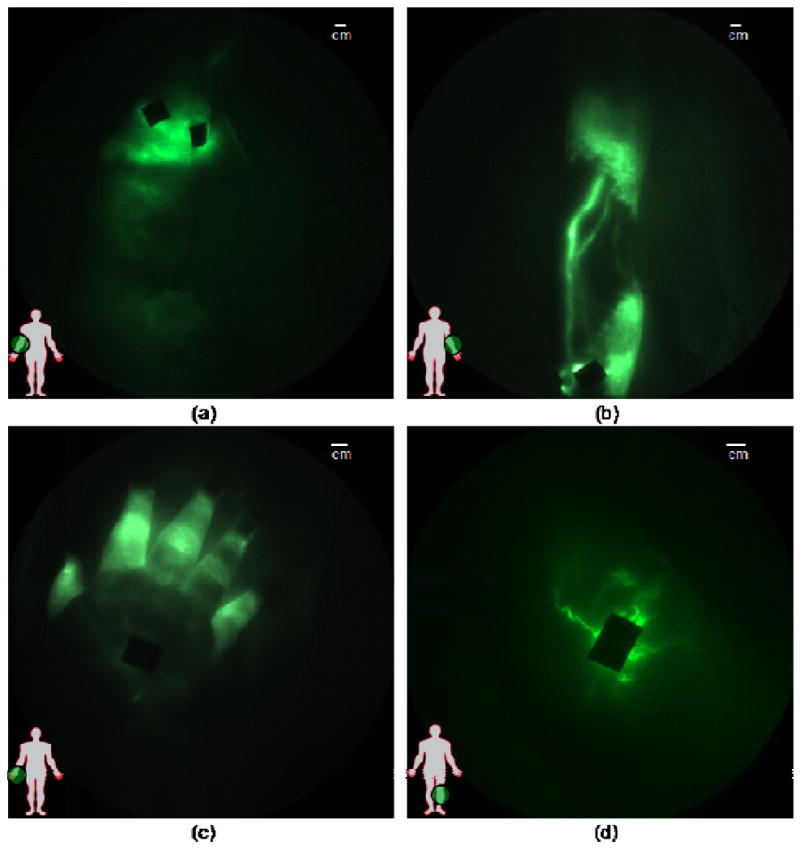
Near-infrared (NIR) fluorescence imaging clinical studies have been reported in the literature with six different devices that employ various doses of indocyanine green (ICG) as a non-specific contrast agent. To date, clinical applications range from (i) angiography, intraoperative assessment of vessel patency, and tumor/metastasis delineation following intravenous administration of ICG, and (ii) imaging lymphatic architecture and function following subcutaneous and intradermal ICG administration. In the latter case, NIR fluorescence imaging may enable new discoveries associated with lymphatic function due to (i) a unique niche that is not met by any other conventional imaging technology and (ii) its exquisite sensitivity enabling high spatial and temporal resolution. Herein, we (i) review the basics of clinical NIR fluorescence imaging, (ii) survey the literature on clinical application of investigational devices using ICG fluorescent contrast, (iii) provide an update of non-invasive dynamic lymphatic imaging conducted with our FDPM device, and finally, (iv) comment on the future NIR fluorescence imaging for non-invasive and intraoperative use given recent demonstrations showing capabilities for imaging following microdose administration of contrast agent.
Figures
References
-
- Alitalo K, Tammela T, Petrova TV. Lymphangiogenesis in development and human disease. Nature. 2005;438(7070):946–53. - PubMed
-
- Rockson SG. Lymphedema. Am J Med. 2001 Mar;110(4):288–95. - PubMed
-
- Armer JM. The problem of post-breast cancer lymphedema: impact and measurement issues. Cancer Invest. 2005;23(1):76–83. - PubMed
-
- Ridner SH. Pretreatment lymphedema education and identified educational resources in breast cancer patients. Patient Educ Couns. 2006;61(1):72–9. - PubMed
-
- Mansel RE, Fallowfield L, Kissin M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC Trial. J Natl Cancer Inst. 2006;98(9):599–609. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous