

Conceptual models for integrating palliative care at cancer centers
- PMID: 22925157
- PMCID: PMC3533890
- DOI: 10.1089/jpm.2012.0147
Conceptual models for integrating palliative care at cancer centers
Abstract
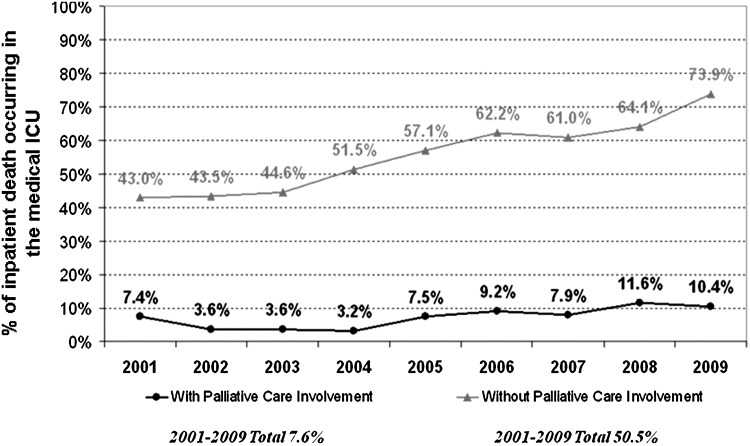
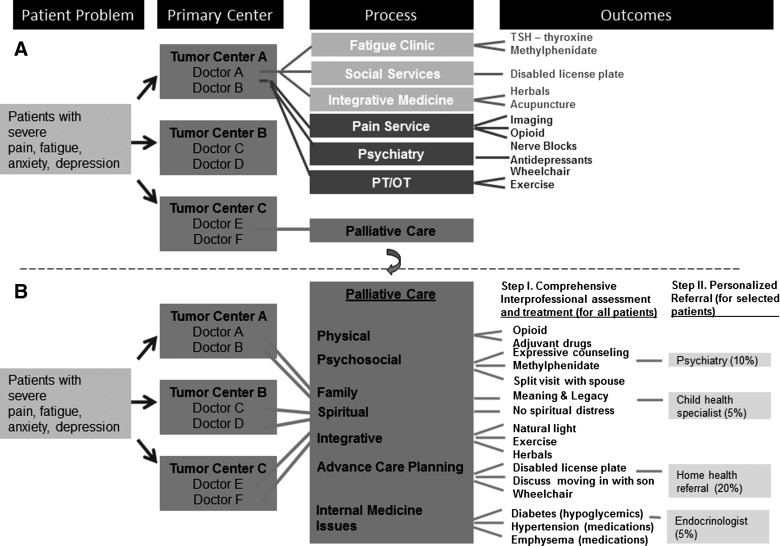
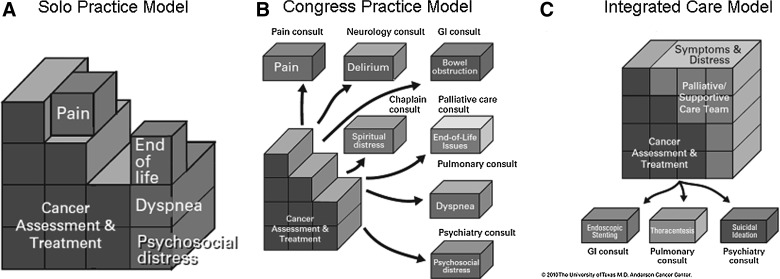
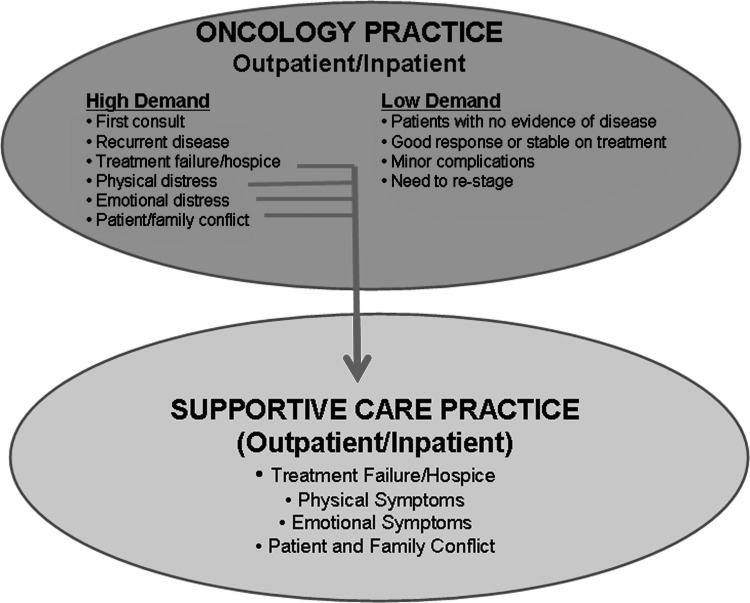
Palliative care programs are rapidly evolving in acute care facilities. Increased and earlier access has been advocated for patients with life-threatening illnesses. Existing programs would need major growth to accommodate the increased utilization. The objective of this review is to provide an update on the current structures, processes, and outcomes of the Supportive and Palliative Care Program at the University of Texas M.D. Anderson Cancer Center (UTMDACC), and to use the update as a platform to discuss the challenges and opportunities in integrating palliative and supportive services in a tertiary care cancer center. Our interprofessional program consists of a mobile consultation team, an acute palliative care unit, and an outpatient supportive care clinic. We will discuss various metrics including symptom outcomes, quality of end-of-life care, program growth, and financial issues. Despite the growing evidence to support early palliative care involvement, referral to palliative care remains heterogeneous and delayed. To address this issue, we will discuss various conceptual models and practical recommendations to optimize palliative care access.
Figures

References
-
- Clark D. von Gunten C. The development of palliative medicine in the UK and Ireland. In: Bruera E, editor; Higginson IJ, editor; Ripamonti R, editor; Textbook of Palliative Medicine. London: Hodder Arnold; 2006. pp. 3–11.
-
- Fukui S. Fujita J. Tsujimura M. Sumikawa Y. Hayashi Y. Fukui N. Late referrals to home palliative care service affecting death at home in advanced cancer patients in Japan: A nationwide survey. Ann Oncol. 2011;22:2113–2120. - PubMed
-
- Teno JM. Shu JE. Casarett D. Spence C. Rhodes R. Connor S. Timing of referral to hospice and quality of care: Length of stay and bereaved family members' perceptions of the timing of hospice referral. J Pain Symptom Manage. 2007;34:120–125. - PubMed
-
- MacDonald N. von Gunten C. The development of palliative care in Canada. In: Bruera E, editor; Higginson IJ, editor; Ripamonti R, editor; Textbook of Palliative Medicine. London: Hodder Arnold; 2006. pp. 22–28.
-
- Meier DE. Beresford L. Outpatient clinics are a new frontier for palliative care. J Palliat Med. 2008;11:823–828. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
