

High throughput measurement of Ca²⁺ dynamics for drug risk assessment in human stem cell-derived cardiomyocytes by kinetic image cytometry
- PMID: 22926323
- PMCID: PMC3667588
- DOI: 10.1016/j.vascn.2012.08.167
High throughput measurement of Ca²⁺ dynamics for drug risk assessment in human stem cell-derived cardiomyocytes by kinetic image cytometry
Abstract
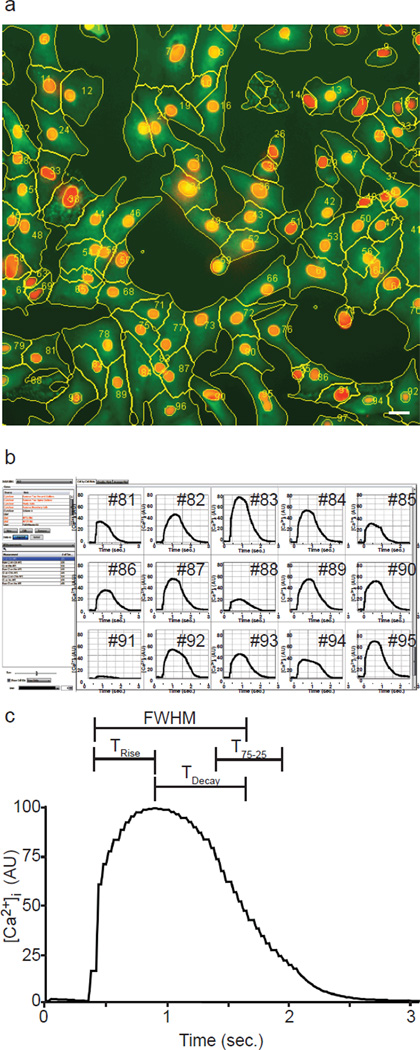
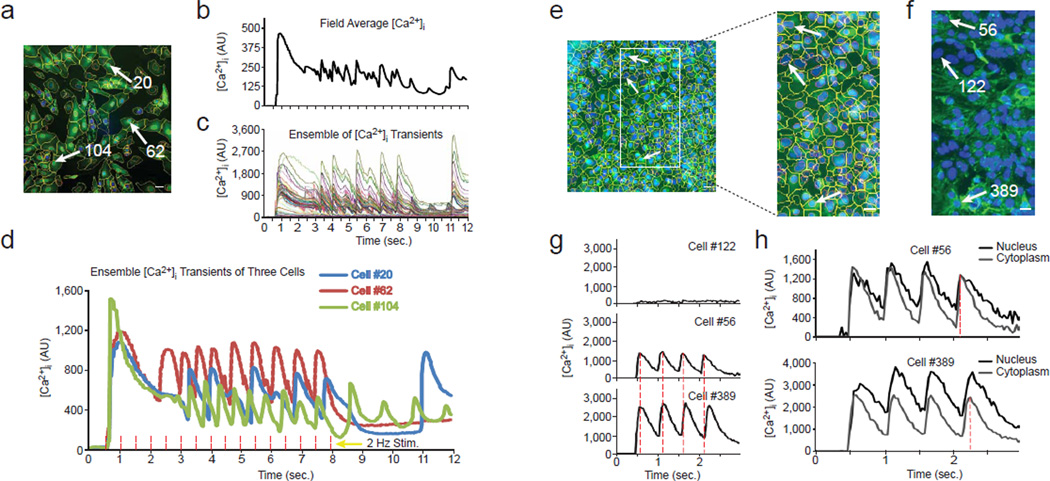
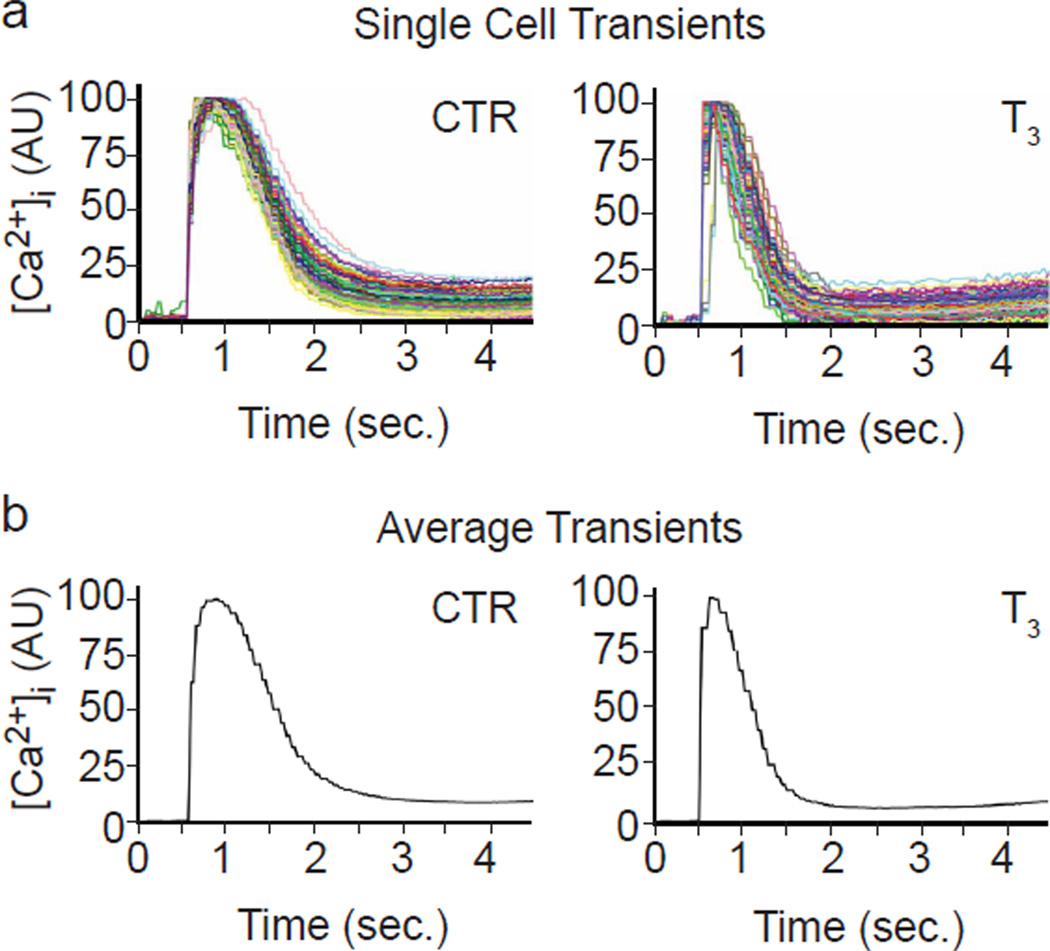
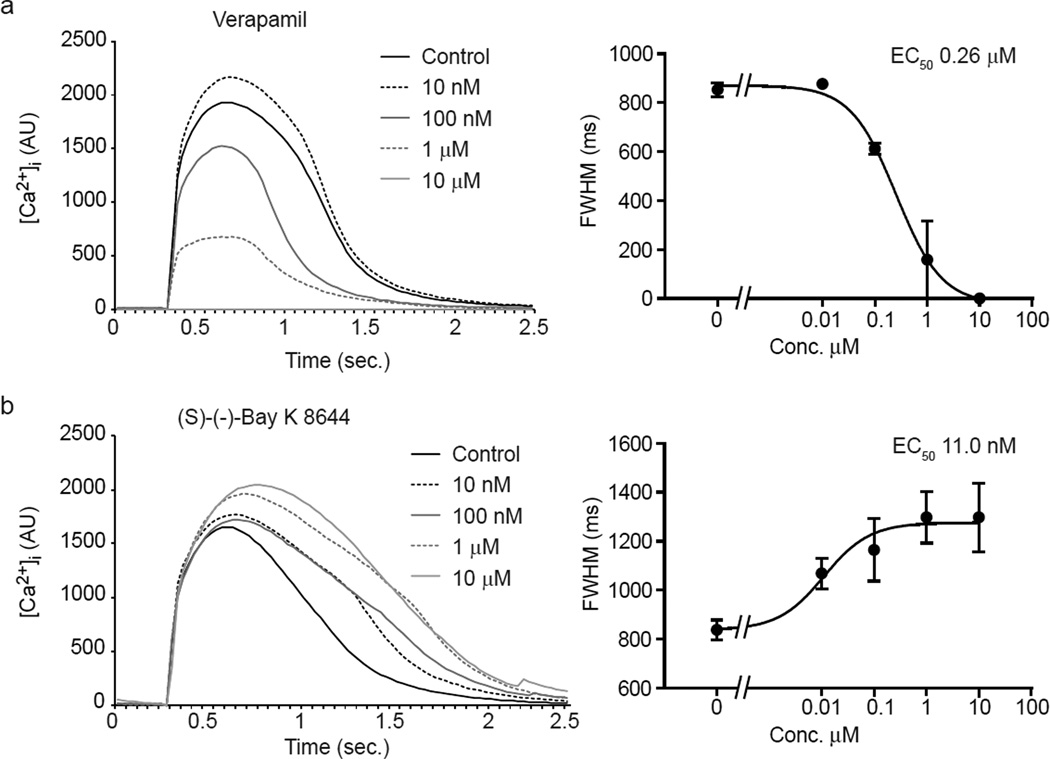
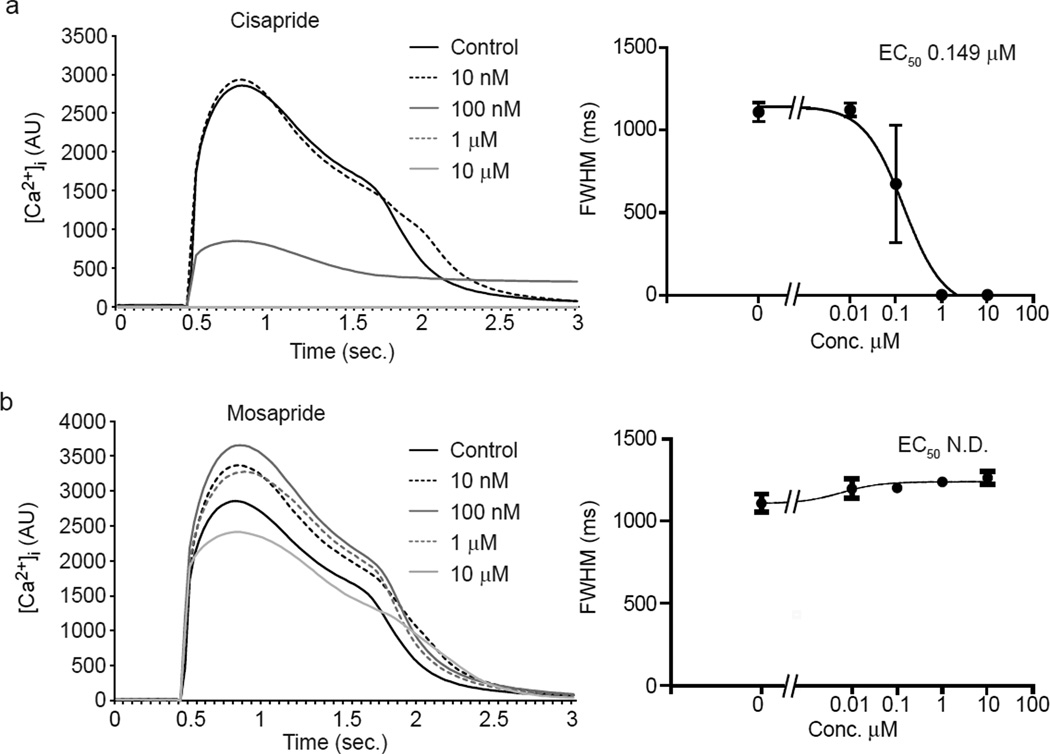
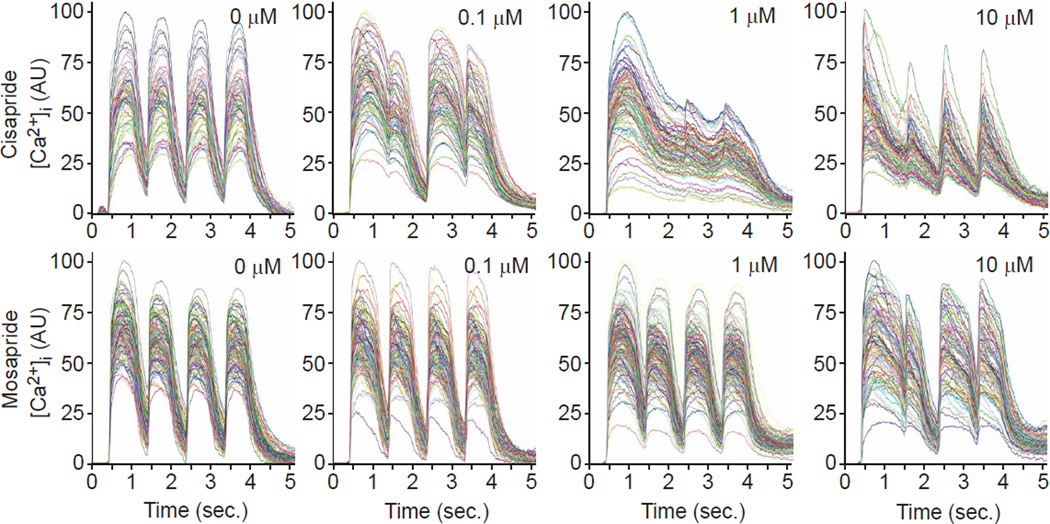
Current methods to measure physiological properties of cardiomyocytes and predict fatal arrhythmias that can cause sudden death, such as Torsade de Pointes, lack either the automation and throughput needed for early-stage drug discovery and/or have poor predictive value. To increase throughput and predictive power of in vitro assays, we developed kinetic imaging cytometry (KIC) for automated cell-by-cell analyses via intracellular fluorescence Ca²⁺ indicators. The KIC instrument simultaneously records and analyzes intracellular calcium concentration [Ca²⁺](i) at 30-ms resolution from hundreds of individual cells/well of 96-well plates in seconds, providing kinetic details not previously possible with well averaging technologies such as plate readers. Analyses of human embryonic stem cell and induced pluripotent stem cell-derived cardiomyocytes revealed effects of known cardiotoxic and arrhythmogenic drugs on kinetic parameters of Ca²⁺ dynamics, suggesting that KIC will aid in the assessment of cardiotoxic risk and in the elucidation of pathogenic mechanisms of heart disease associated with drugs treatment and/or genetic background.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Antzelevitch C. Arrhythmogenic mechanisms of QT prolonging drugs: Is QT prolongation really the problem? Journal of Electrocardiology. 2004;37:15–24. - PubMed
-
- Balasubramaniam R, Chawla S, Grace AA, Huang CLH. Caffeine-induced arrhythmias in murine hearts parallel changes in cellular Ca2+ homeostasis. Am J Physiol Heart Circ Physiol. 2005;289:1584–1593. - PubMed
-
- Bers DM. Cardiac excitation-contraction coupling. Nature. 2002;415:198–205. - PubMed
-
- Bode G, Olejniczak K. ICH Topic: The draft ICH S7B step 2: Note for guidance on safety pharmacology studies for human pharmaceuticals. Fundamental & Clinical Pharmacology. 2002;16:105–118. - PubMed
-
- Bootman MD, Fearnley C, Smyrnias I, MacDonald F, Roderick HL. An update on nuclear calcium signalling. J Cell Sci. 2009;122:2337–2350. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
