

Early antipyretic exposure does not increase mortality in patients with gram-negative severe sepsis: a retrospective cohort study
- PMID: 22926744
- PMCID: PMC3510482
- DOI: 10.1007/s11739-012-0848-z
Early antipyretic exposure does not increase mortality in patients with gram-negative severe sepsis: a retrospective cohort study
Abstract
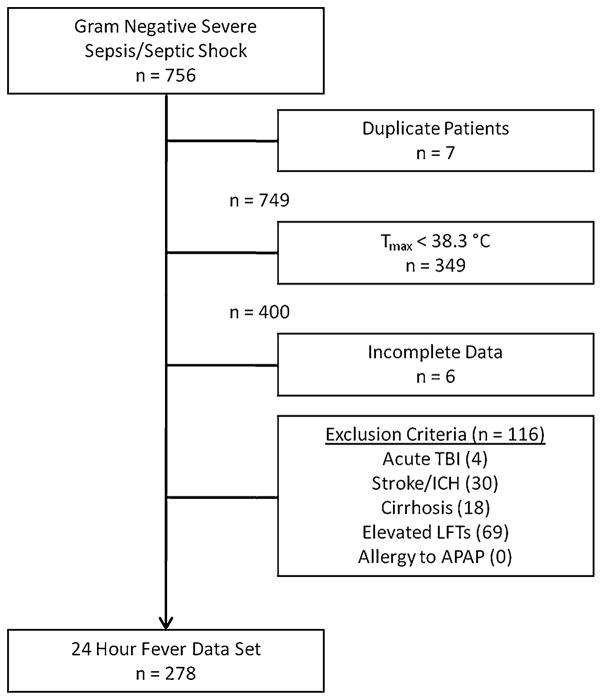
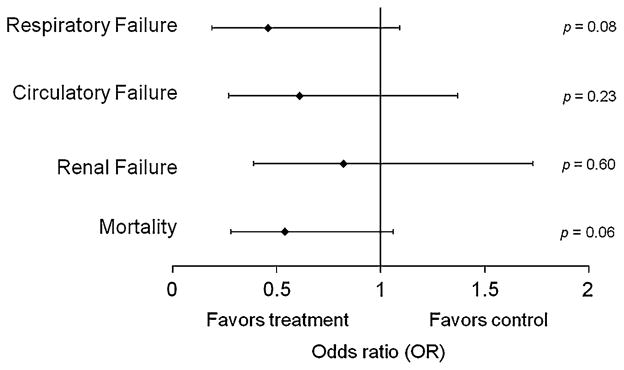
Existing data suggest that antipyretic medications may have deleterious effects on immune function and may increase mortality in human infection. This study was designed to evaluate the impact of antipyretic therapy on 28-day in-hospital mortality when administered early in the course of gram-negative severe sepsis or septic shock. This study was a single-center retrospective cohort study at a 1,111-bed academic medical center of all febrile patients with gram-negative bacteremia hospitalized with severe sepsis or septic shock (n = 278) between Jan 2002 and Feb 2008. Although the raw mortality was lower in the group that received an early antipyretic medication (22 vs. 35 %, p = 0.01), patients in the early antipyretic group had higher mean arterial pressure (58.0 vs. 52.7, p = 0.01) and higher 24-h T (max) (39.3 vs. 39.0, p < 0.01). Early antipyretic therapy was not significantly associated with 28-day in-hospital mortality (adjusted OR 0.55, 0.29-1.03) in a multivariable logistic regression model controlling for APACHE-II score, hypotension, pneumonia, surgery during hospitalization, persistent fever, and in-hospital dialysis. In conclusion, early antipyretic therapy is not associated with increased mortality.
Conflict of interest statement
Figures
Similar articles
-
Clinical and demographic factors associated with antipyretic use in gram-negative severe sepsis and septic shock.Ann Pharmacother. 2011 Oct;45(10):1207-16. doi: 10.1345/aph.1Q319. Epub 2011 Sep 20. Ann Pharmacother. 2011. PMID: 21934034 Free PMC article.
-
Association of body temperature and antipyretic treatments with mortality of critically ill patients with and without sepsis: multi-centered prospective observational study.Crit Care. 2012 Feb 28;16(1):R33. doi: 10.1186/cc11211. Crit Care. 2012. PMID: 22373120 Free PMC article. Clinical Trial.
-
Multi-drug resistance, inappropriate initial antibiotic therapy and mortality in Gram-negative severe sepsis and septic shock: a retrospective cohort study.Crit Care. 2014 Nov 21;18(6):596. doi: 10.1186/s13054-014-0596-8. Crit Care. 2014. PMID: 25412897 Free PMC article.
-
Combined and alternating paracetamol and ibuprofen therapy for febrile children.Evid Based Child Health. 2014 Sep;9(3):675-729. doi: 10.1002/ebch.1978. Evid Based Child Health. 2014. PMID: 25236309 Review.
-
Dosing and antipyretic efficacy of oral acetaminophen in children.Clin Ther. 2013 Sep;35(9):1361-75.e1-45. doi: 10.1016/j.clinthera.2013.06.022. Epub 2013 Aug 23. Clin Ther. 2013. PMID: 23972576 Review.
Cited by
-
Early acetaminophen Use and 90-day mortality in ICU patients with ischemic stroke.Front Pharmacol. 2025 Jul 24;16:1622440. doi: 10.3389/fphar.2025.1622440. eCollection 2025. Front Pharmacol. 2025. PMID: 40777988 Free PMC article.
-
Fever Is Associated with Reduced, Hypothermia with Increased Mortality in Septic Patients: A Meta-Analysis of Clinical Trials.PLoS One. 2017 Jan 12;12(1):e0170152. doi: 10.1371/journal.pone.0170152. eCollection 2017. PLoS One. 2017. PMID: 28081244 Free PMC article.
-
The modern pharmacology of paracetamol: therapeutic actions, mechanism of action, metabolism, toxicity and recent pharmacological findings.Inflammopharmacology. 2013 Jun;21(3):201-32. doi: 10.1007/s10787-013-0172-x. Epub 2013 May 30. Inflammopharmacology. 2013. PMID: 23719833 Review.
-
Antipyretic Therapy in Critically Ill Septic Patients: A Systematic Review and Meta-Analysis.Crit Care Med. 2017 May;45(5):806-813. doi: 10.1097/CCM.0000000000002285. Crit Care Med. 2017. PMID: 28221185 Free PMC article.
-
Antipyretic therapy in critically ill patients with sepsis: an interaction with body temperature.PLoS One. 2015 Mar 30;10(3):e0121919. doi: 10.1371/journal.pone.0121919. eCollection 2015. PLoS One. 2015. PMID: 25822614 Free PMC article.
References
-
- Arons MM, Wheeler AP, Bernard GR, Christman BW, Russell JA, Schein R, Summer WR, Steinberg KP, Fulkerson W, Wright P, Dupont WD, Swindell BB. Effects of ibuprofen on the physiology and survival of hypothermic sepsis. Crit Care Med. 1999;27(4):699–707. - PubMed
-
- Kluger MJ, Ringler DH, Anver MR. Fever and survival. Science. 1975;188(4184):166–168. - PubMed
-
- Bernheim HA, Kluger MJ. Fever: effect of drug-induced antipyresis on survival. Science. 1976;193(4249):237–239. - PubMed
-
- Su F, Nguyen ND, Wang Z, Cai Y, Rogiers P, Vincent JL. Fever control in septic shock: beneficial or harmful? Shock. 2005;23(6):516–520. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
