

Relationship of surgical accuracy and clinical outcomes in Charitè lumbar disc replacement
- PMID: 22927148
- PMCID: PMC6583509
- DOI: 10.1111/j.1757-7861.2012.00191.x
Relationship of surgical accuracy and clinical outcomes in Charitè lumbar disc replacement
Abstract
Objective: To retrospectively assess the clinical and functional outcomes of a group of patients receiving Charitè lumbar disc replacement and to compare those outcomes to the corresponding surgical technical accuracy.
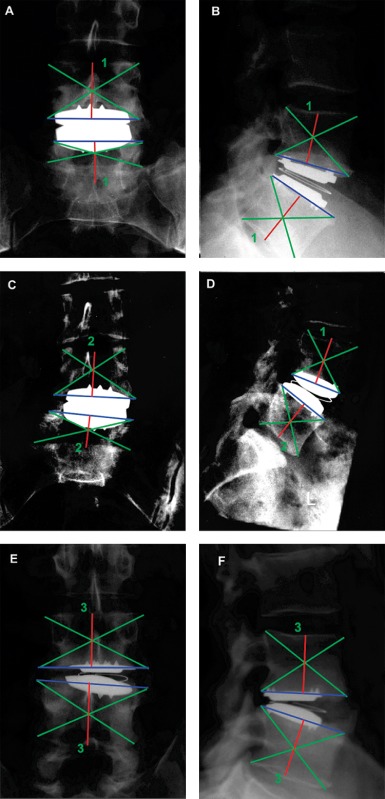
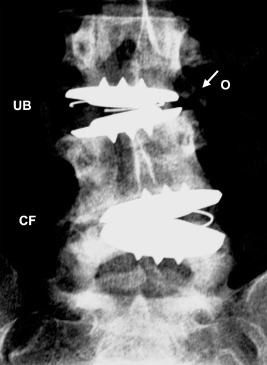
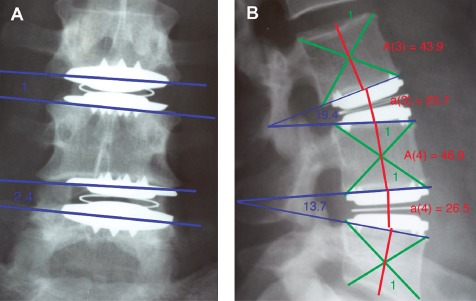
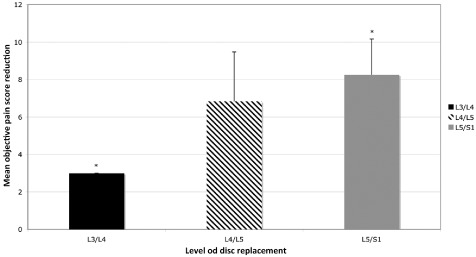
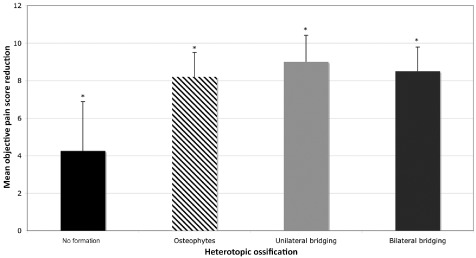
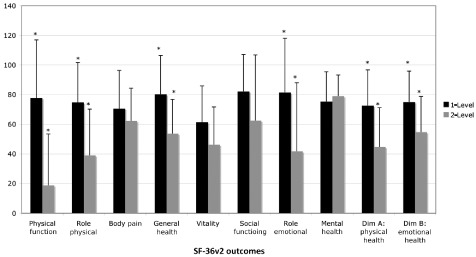
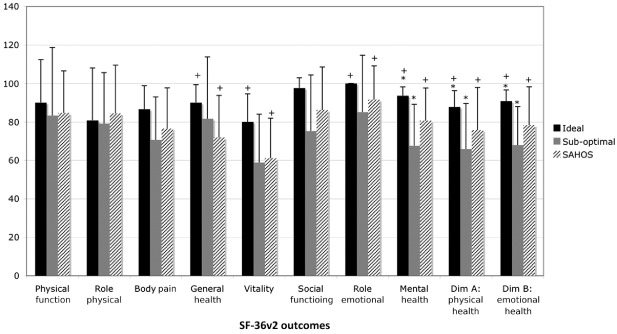
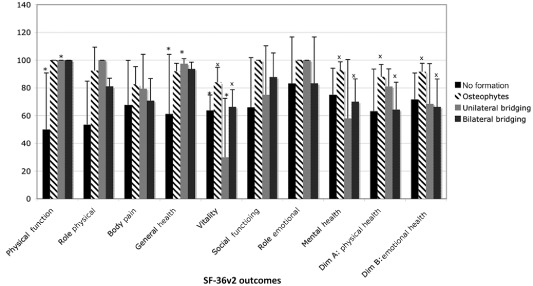
Methods: A retrospective study of all patients treated over a 3-year period was undertaken. Objective pain scores were quantified from 1 to 10. Short Form 36-Health Survey (SF-36v2) scores were compared to Australian population norms. Surgical placements were radiographically classified. Heterotopic ossification, disc height restoration and angle-defined instability were assessed using established protocols.
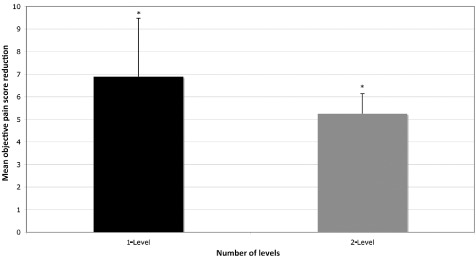
Results: Twenty-five patients were identified with three patients lost to follow-up. Average follow-up was 34 months. Ideal surgical placement was achieved in five (33%) single-level and three (37.5%) dual-level disc replacements. Sub-optimal surgical placement was seen in nine (60%) single-level and five (62.5%) dual-level disc replacements. Poor surgical placement was observed in a single-level disc replacement. All patients demonstrated a reduction in objective pain score (P < 0.05). SF-36v2 outcomes were superior in single-level compared to dual-level and ideal compared to sub-optimal replacements (P < 0.05).
Conclusion: The hypothesis that ideal surgical placements are associated with improved clinical and functional outcomes in total lumbar disc replacement was confirmed.
© 2012 Tianjin Hospital and Wiley Publishing Asia Pty Ltd.
Figures
Similar articles
-
A prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part II: evaluation of radiographic outcomes and correlation of surgical technique accuracy with clinical outcomes.Spine (Phila Pa 1976). 2005 Jul 15;30(14):1576-83; discussion E388-90. doi: 10.1097/01.brs.0000170561.25636.1c. Spine (Phila Pa 1976). 2005. PMID: 16025025 Clinical Trial.
-
An 11-year minimum follow-up of the Charite III lumbar disc replacement for the treatment of symptomatic degenerative disc disease.Eur Spine J. 2015 Sep;24(9):2056-64. doi: 10.1007/s00586-015-3939-5. Epub 2015 Apr 21. Eur Spine J. 2015. PMID: 25895882
-
A prospective, randomized, multicenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part I: evaluation of clinical outcomes.Spine (Phila Pa 1976). 2005 Jul 15;30(14):1565-75; discussion E387-91. doi: 10.1097/01.brs.0000170587.32676.0e. Spine (Phila Pa 1976). 2005. PMID: 16025024 Clinical Trial.
-
Mid- to long-term results of total disc replacement for lumbar degenerative disc disease: a systematic review.J Orthop Surg Res. 2018 Dec 26;13(1):326. doi: 10.1186/s13018-018-1032-6. J Orthop Surg Res. 2018. PMID: 30585142 Free PMC article.
-
Lumbar total disc replacement. Surgical technique.J Bone Joint Surg Am. 2006 Mar;88 Suppl 1 Pt 1:50-64. doi: 10.2106/JBJS.E.01066. J Bone Joint Surg Am. 2006. PMID: 16510800 Review.
Cited by
-
Lumbar total disc arthroplasty: outdated surgery or here to stay procedure? A systematic review of current literature.J Orthop Traumatol. 2017 Sep;18(3):197-215. doi: 10.1007/s10195-017-0462-y. Epub 2017 Jul 6. J Orthop Traumatol. 2017. PMID: 28685344 Free PMC article.
-
We Need to Talk about Lumbar Total Disc Replacement.Int J Spine Surg. 2018 Aug 3;12(2):201-240. doi: 10.14444/5029. eCollection 2018 Apr. Int J Spine Surg. 2018. PMID: 30276080 Free PMC article.
-
Impact of heterotopic ossification following lumbar total disk replacement: a systematic review.BMC Musculoskelet Disord. 2022 Apr 23;23(1):382. doi: 10.1186/s12891-022-05322-9. BMC Musculoskelet Disord. 2022. PMID: 35461244 Free PMC article.
-
Novel use of robotics and navigation for anterior lumbar total disc replacement surgery.N Am Spine Soc J. 2022 Jan 5;9:100097. doi: 10.1016/j.xnsj.2021.100097. eCollection 2022 Mar. N Am Spine Soc J. 2022. PMID: 35141661 Free PMC article.
-
ISASS Policy Statement - Lumbar Artificial Disc.Int J Spine Surg. 2015 Mar 12;9:7. doi: 10.14444/2007. eCollection 2015. Int J Spine Surg. 2015. PMID: 25785243 Free PMC article.
References
-
- Bao QB, Yuan HA. Prosthetic disc replacement: the future? Clin Orthop Relat Res, 2002, 394: 139–145. - PubMed
-
- German JW, Foley KT. Disc arthroplasty in the management of the painful lumbar motion segment. Spine, 2005, 30 (16 Suppl.): S60–S67. - PubMed
-
- Lemaire JP, Carrier H, Sariali H, et al Clinical and radiological outcomes with the Charité artificial disc: a 10‐year minimum follow‐up. J Spinal Disord Tech, 2005, 18: 353–359. - PubMed
-
- Blumenthal S, McAfee PC, Guyer RD, et al A prospective, randomized, multicenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part I: evaluation of clinical outcomes. Spine, 2005, 30: 1565–1575. - PubMed
-
- Blumenthal SL, Ohnmeiss DD, Guyer RD, et al Prospective study evaluating total disc replacement: preliminary results. J Spinal Disord Tech, 2003, 16: 450–454. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
