

Cognitive outcomes following contemporary treatment without cranial irradiation for childhood acute lymphoblastic leukemia
- PMID: 22927505
- PMCID: PMC3529594
- DOI: 10.1093/jnci/djs344
Cognitive outcomes following contemporary treatment without cranial irradiation for childhood acute lymphoblastic leukemia
Abstract
Background: Treatment of acute lymphoblastic leukemia (ALL) has included the use of prophylactic cranial irradiation in up to 20% of children with high-risk disease despite known cognitive risks of this treatment modality.
Methods: Patients enrolled on the St Jude ALL Total Therapy Study XV, which omitted prophylactic cranial irradiation in all patients, were assessed 120 weeks after completion of consolidation therapy (n = 243) using a comprehensive cognitive battery. χ(2) analysis was used to compare the percentage of below-average performers among the entire ALL patient group to the expected rate based on the normative sample. Univariate logistic regression was used to estimate the effect of intensity of chemotherapy (treatment arm), age at diagnosis, and sex on the probability of below-average performance. All statistical tests were two-sided.
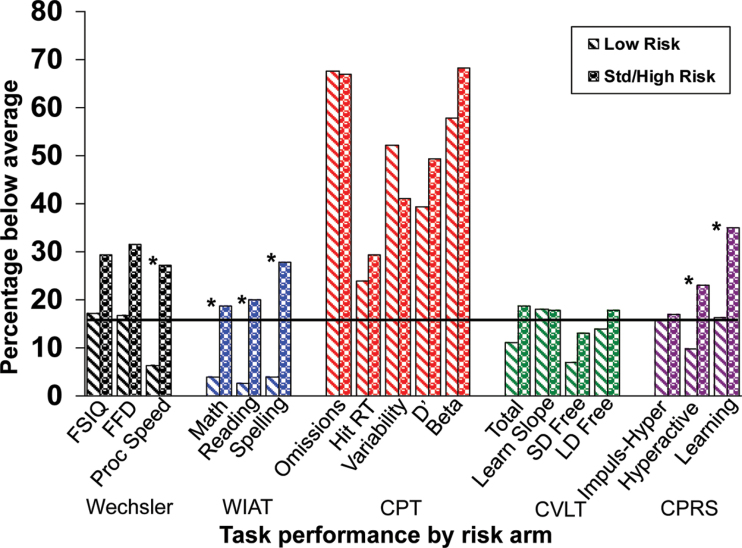
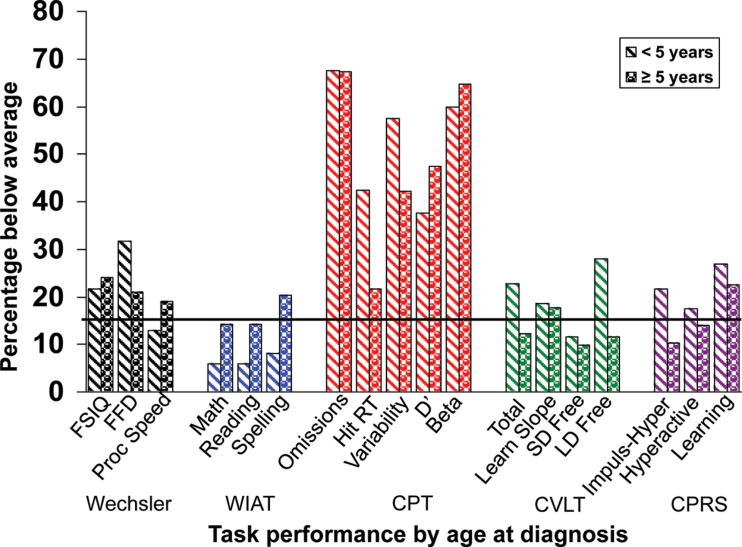
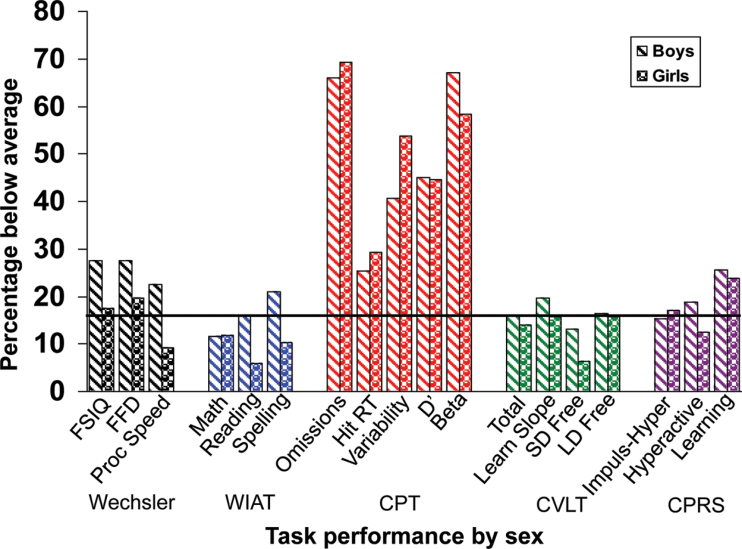
Results: Overall, the ALL group had a statistically significantly higher risk for below-average performance on a measure of sustained attention (67.31% more than 1 SD below the normative mean for omission errors, P < .001) but not on measures of intellectual functioning, academic skills, or memory. Patients given higher intensity chemotherapy were at greater risk for below-average performance compared with those given lower intensity therapy on measures of processing speed (27.14% vs 6.25%, P = .009) and academic abilities (Math Reasoning: 18.60% vs 3.90%, P = .008; Word Reading: 20.00% vs 2.60%, P = .007; Spelling: 27.91% vs 3.90%, P = .001) and had higher parent-reported hyperactivity (23.00% vs 9.84%, P = .018) and learning problems (35.00% vs 16.39%, P = .005). Neither age at diagnosis nor sex was associated with risk for below-average cognitive performance.
Conclusions: Omitting cranial irradiation may help preserve global cognitive abilities, but treatment with chemotherapy alone is not without risks. Caregiver education and development of interventions should address both early attention deficits and cognitive late effects.
Figures
References
-
- Moricke A, Reiter A, Zimmermann M, et al. Risk-adjusted therapy of acute lymphoblastic leukemia can decrease treatment burden and improve survival: treatment results of 2169 unselected pediatric and adolescent patients enrolled in the trial ALL_BFM 95 Blood. 2008;111(9):4477–4489 - PubMed
-
- Pui CH, Sandlund JT, Pei D, et al. Improved outcome for children with acute lymphoblastic leukemia: results of Total Therapy Study XIIIB at St Jude Children’s Research Hospital Blood. 2004;104(9):2690–2696 - PubMed
-
- Copeland DR, Fletcher JM, Pfefferbaum-Levine B, et al. Neuropsychological sequelae of childhood cancer in long-term survivors Pediatrics. 1985;75:745–753 - PubMed
-
- Rowland JH, Glidewell OJ, Sibley RF, et al. Effects of different forms of central nervous system prophylaxis on neuropsychologic function in childhood leukemia J Clin Oncol. 1984;2(12):1327–1335 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
