

Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: a systematic review and meta-analysis
- PMID: 22927798
- PMCID: PMC3424246
- DOI: 10.1371/journal.pmed.1001293
Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: a systematic review and meta-analysis
Abstract
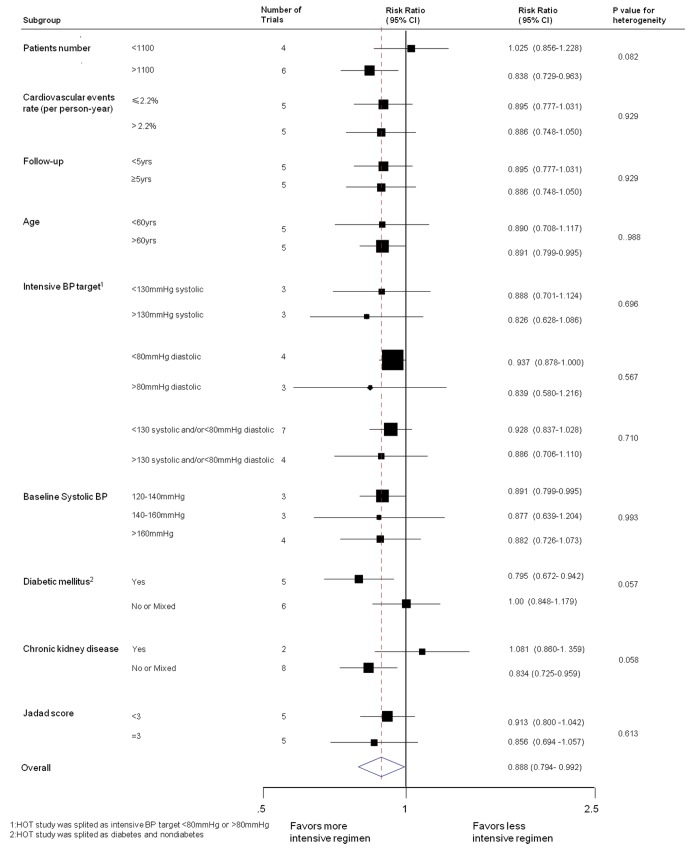
Background: Guidelines recommend intensive blood pressure (BP) lowering in patients at high risk. While placebo-controlled trials have demonstrated 22% reductions in coronary heart disease (CHD) and stroke associated with a 10-mmHg difference in systolic BP, it is unclear if more intensive BP lowering strategies are associated with greater reductions in risk of CHD and stroke. We did a systematic review to assess the effects of intensive BP lowering on vascular, eye, and renal outcomes.
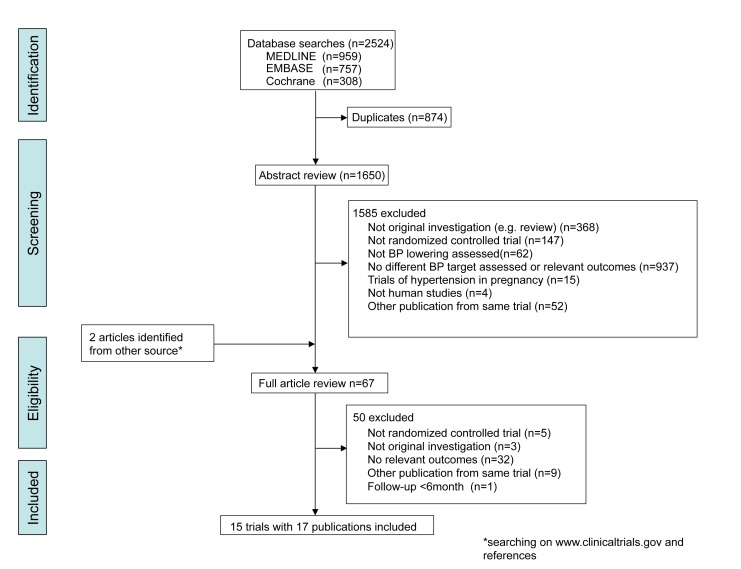
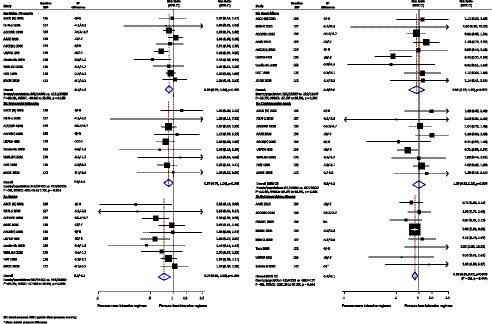
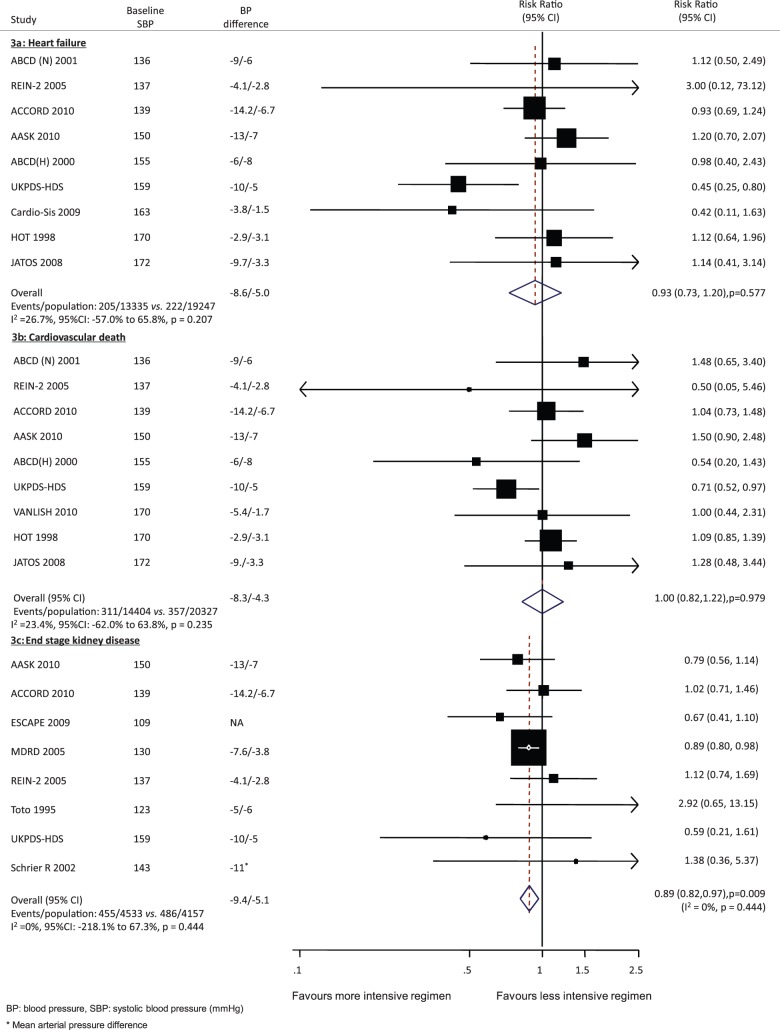
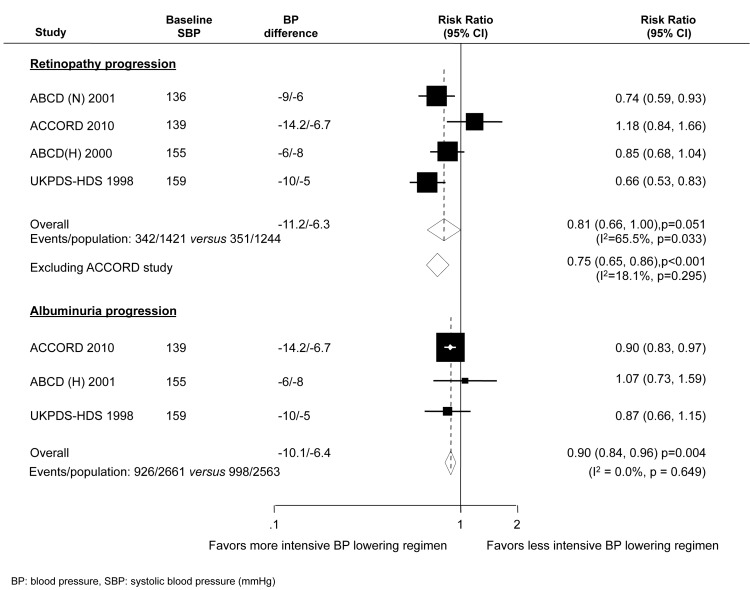
Methods and findings: We systematically searched Medline, Embase, and the Cochrane Library for trials published between 1950 and July 2011. We included trials that randomly assigned individuals to different target BP levels. We identified 15 trials including a total of 37,348 participants. On average there was a 7.5/4.5-mmHg BP difference. Intensive BP lowering achieved relative risk (RR) reductions of 11% for major cardiovascular events (95% CI 1%-21%), 13% for myocardial infarction (0%-25%), 24% for stroke (8%-37%), and 11% for end stage kidney disease (3%-18%). Intensive BP lowering regimens also produced a 10% reduction in the risk of albuminuria (4%-16%), and a trend towards benefit for retinopathy (19%, 0%-34%, p = 0.051) in patients with diabetes. There was no clear effect on cardiovascular or noncardiovascular death. Intensive BP lowering was well tolerated; with serious adverse events uncommon and not significantly increased, except for hypotension (RR 4.16, 95% CI 2.25 to 7.70), which occurred infrequently (0.4% per 100 person-years).
Conclusions: Intensive BP lowering regimens provided greater vascular protection than standard regimens that was proportional to the achieved difference in systolic BP, but did not have any clear impact on the risk of death or serious adverse events. Further trials are required to more clearly define the risks and benefits of BP targets below those currently recommended, given the benefits suggested by the currently available data.
Conflict of interest statement
JL has received grant support from Pfizer for hypertension research. VP, MW, SM, and JC have received honoraria from Servier for scientific presentations relating to blood pressure. SM and JC were principal investigators on ADVANCE, a blood pressure lowering trial funded by Servier and the Australian National Health and Medical Research Council. BN has received BP-related research support from Servier, and honoraria for scientific presentations related to blood pressure from Novartis, Tanabe, and Servier. AR has received an unrestricted grant from Dr Reddy’s Laboratories for a trial that includes blood pressure-lowering agents. PE, FT, TN, HW, and GH declare they have no competing interests.
Figures
References
-
- MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, et al. (1990) Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 335: 765–774. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R (2002) Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 360: 1903–1913. - PubMed
-
- Lawes CM, Rodgers A, Bennett DA, Parag V, Suh I, et al. (2003) Blood pressure and cardiovascular disease in the Asia Pacific region. J Hypertens 21: 707–716. - PubMed
-
- Turnbull F (2003) Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet 362: 1527–1535. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
