

The place of immunotherapy in the management of HCV-induced vasculitis: an update
- PMID: 22927871
- PMCID: PMC3426208
- DOI: 10.1155/2012/315167
The place of immunotherapy in the management of HCV-induced vasculitis: an update
Abstract
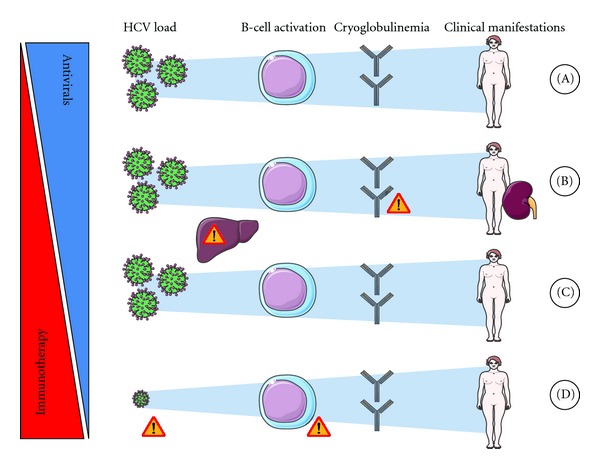
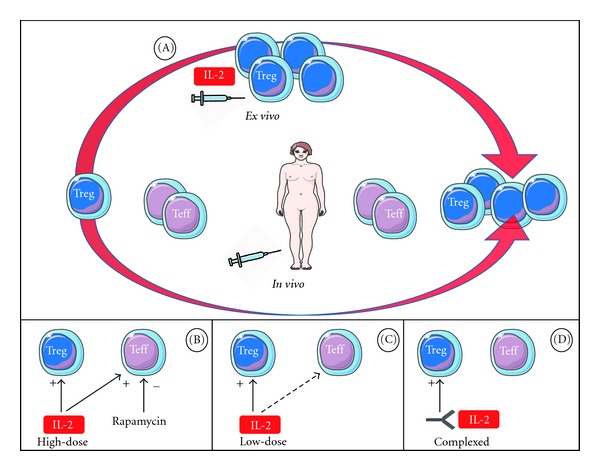
Patients with chronic hepatitis C virus (HCV) can develop systemic cryoglobulinemic vasculitis. Combination of pegylated-interferon α and ribavirin is the first-line treatment of this condition. However, in case of severe or life-threatening manifestations, absence of a virological response, or autonomized vasculitis, immunotherapy (alone or in addition to the antiviral regimen) is necessary. Rituximab is to date the only biologic with a sufficient level of evidence to support its use in this indication. Several studies have demonstrated that rituximab is highly effective when cryoglobulinaemic vasculitis is refractory to antiviral regimen, that association of rituximab with antiviral regimen may induce a better and faster clinical remission, and, recently, that rituximab is more efficient than traditional immunosuppressive treatments. Some issues with regard to the optimal dose of rituximab or its use as maintenance treatment remain unsolved. Interestingly, in balance with this anti-inflammatory strategy, a recent pilot study reported the significant expansion of circulating regulatory T lymphocytes with concomitant clinical improvement in patients with refractory HCV-induced cryoglobulinaemic vasculitis using low dose of subcutaneous interleukin-2. This paper provides an updated overview on the place of immunotherapy, especially biologics, in the management of HCV-induced cryoglobulinaemic vasculitis.
Figures
References
-
- Landau DA, Scerra S, Sene D, Resche-Rigon M, Saadoun D, Cacoub P. Causes and predictive factors of mortality in a cohort of patients with hepatitis C virus-related cryoglobulinemic vasculitis treated with antiviral therapy. Journal of Rheumatology. 2010;37(3):615–621. - PubMed
-
- Manns MP, McHutchison JG, Gordon SC, et al. Peginterferon alfa-2b plus ribavirin compared with interferonalfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a randomised trial. The Lancet. 2001;358(9286):958–965. - PubMed
-
- Fried MW, Shiffman ML, Rajender Reddy K, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. New England Journal of Medicine. 2002;347(13):975–982. - PubMed
-
- Hadziyannis SJ, Sette H, Morgan TR, et al. Peginterferon-α2a and ribavirin combination therapy in chronic hepatitis C: a randomized study of treatment duration and ribavirin dose. Annals of Internal Medicine. 2004;140(5):346–I67. - PubMed
-
- Cavallo R, Roccatello D, Menegatti E, Naretto C, Napoli F, Baldovino S. Rituximab in cryoglobulinemic peripheral neuropathy. Journal of Neurology. 2009;256(7):1076–1082. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
