

Influencing factors on the NMP-22 urine assay: an experimental model
- PMID: 22928931
- PMCID: PMC3480828
- DOI: 10.1186/1471-2490-12-23
Influencing factors on the NMP-22 urine assay: an experimental model
Abstract
Background: The commercial NMP-22 urine assays for bladder cancer (BCa) detect nuclear mitotic apparatus protein 1 (NUMA1) using monoclonal antibodies. It remains unclear whether these assays are monitoring a tumor antigen or some other phenomenon associated with the disease state. In this study, we investigated the influence of urinary cellular and protein concentration, and hematuria on the performance of the NMP-22 tests in an experimental model.
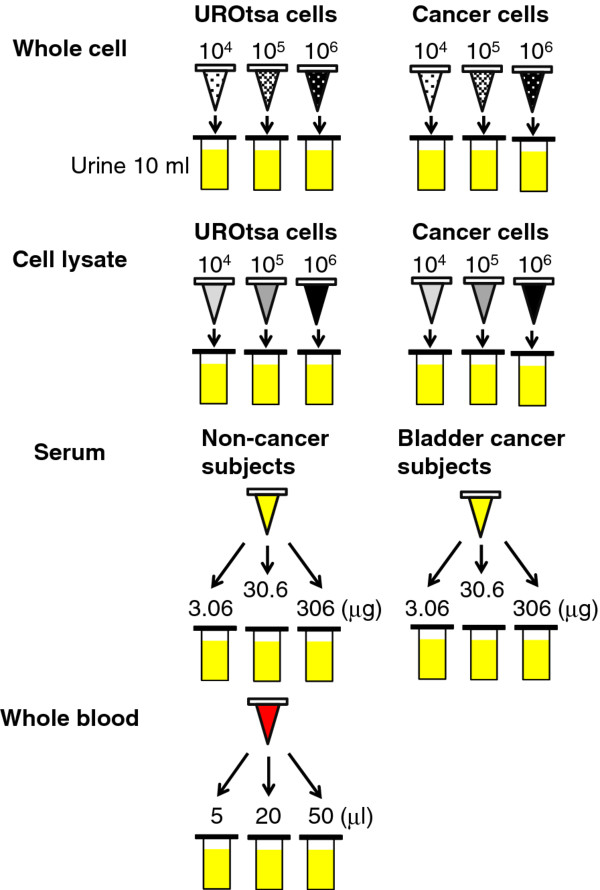
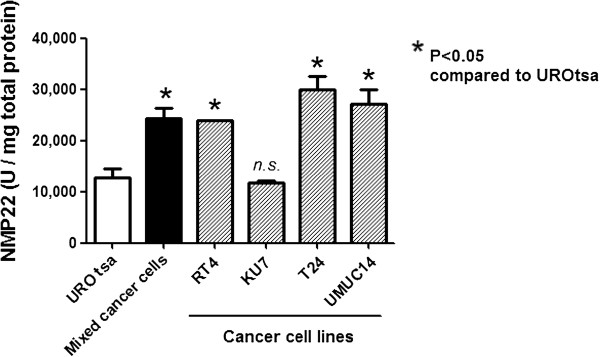
Methods: Pooled urine from healthy subjects were spiked with varying concentrations of benign (UROtsa) cells, cancer cells (RT4, T24, KU-7 and UM-UC-14), whole blood or serum, prior to analysis with both NMP22® Bladder Cancer ELISA test and the NMP22® BladderChek® point-of-care test.
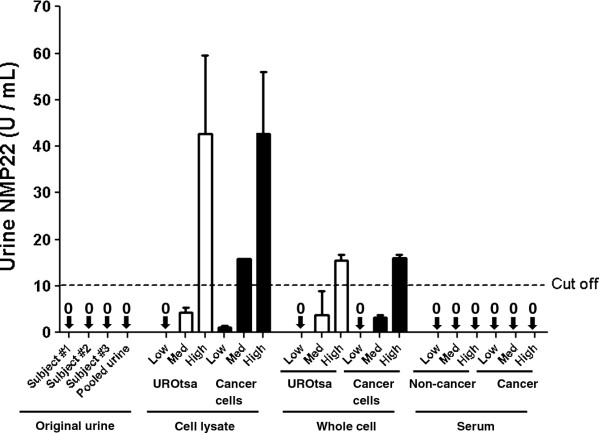
Results: Urines from control subjects were negative for NMP-22. The addition of whole blood at 50ul/10 ml, but not serum, resulted in a false-positive result. Furthermore, the addition of a high concentration of benign urothelial cells (10(6)) or the cell lysate from these cells (306 μg protein) resulted in a false-positive result. High concentrations of pooled-cancer cells (10(6)) or cell lysate (30.6 μg and above) resulted in a positive NMP-22 assay. Concordance between the NMP-22 ELISA assay and the NMP-22 point of care assay was >90%.
Conclusions: Rather than detecting a specific tumor antigen, urinary NMP-22 assays may be measuring the cellularity or amount of cell turnover that may be introduced into the urine by a variety of conditions, including surface shedding from bladder tumors. The absence of significant urinary cellularity in some cases due to lesion characteristics or the timing of sampling may result in false-negative NMP-2 assays.
Figures
References
-
- Rife CC, Farrow GM, Utz DC. Urine cytology of transitional cell neoplasms. Urol Clin North Am. 1979;6:599–612. - PubMed
-
- Kinders R, Jones T, Root R. Complement factor H or a related protein is a marker for transitional cell cancer of the bladder. ClinCancer Res. 1998;4(10):2511–20. - PubMed
-
- Thomas L, Leyh H, Marberger M. et al.Multicenter trial of the quantitative BTA TRAK assay in the detection of bladder cancer. Clin Chem. 1999;45:472–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
