

Current status of boron neutron capture therapy of high grade gliomas and recurrent head and neck cancer
- PMID: 22929110
- PMCID: PMC3583064
- DOI: 10.1186/1748-717X-7-146
Current status of boron neutron capture therapy of high grade gliomas and recurrent head and neck cancer
Abstract
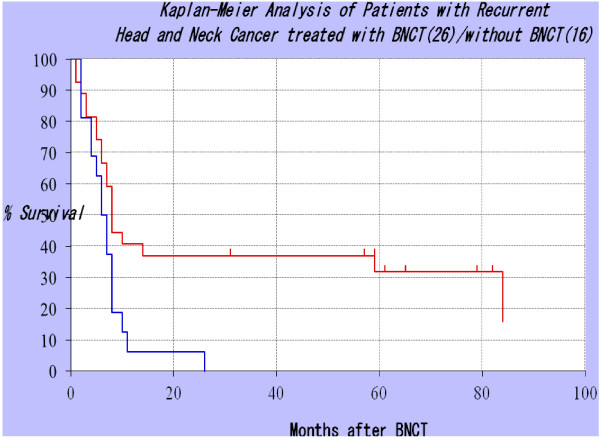
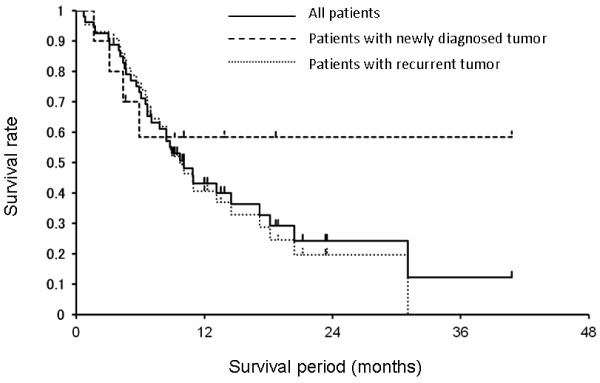
Boron neutron capture therapy (BNCT) is a biochemically targeted radiotherapy based on the nuclear capture and fission reactions that occur when non-radioactive boron-10, which is a constituent of natural elemental boron, is irradiated with low energy thermal neutrons to yield high linear energy transfer alpha particles and recoiling lithium-7 nuclei. Clinical interest in BNCT has focused primarily on the treatment of high grade gliomas, recurrent cancers of the head and neck region and either primary or metastatic melanoma. Neutron sources for BNCT currently have been limited to specially modified nuclear reactors, which are or until the recent Japanese natural disaster, were available in Japan, United States, Finland and several other European countries, Argentina and Taiwan. Accelerators producing epithermal neutron beams also could be used for BNCT and these are being developed in several countries. It is anticipated that the first Japanese accelerator will be available for therapeutic use in 2013. The major hurdle for the design and synthesis of boron delivery agents has been the requirement for selective tumor targeting to achieve boron concentrations in the range of 20 μg/g. This would be sufficient to deliver therapeutic doses of radiation with minimal normal tissue toxicity. Two boron drugs have been used clinically, a dihydroxyboryl derivative of phenylalanine, referred to as boronophenylalanine or "BPA", and sodium borocaptate or "BSH" (Na2B12H11SH). In this report we will provide an overview of other boron delivery agents that currently are under evaluation, neutron sources in use or under development for BNCT, clinical dosimetry, treatment planning, and finally a summary of previous and on-going clinical studies for high grade gliomas and recurrent tumors of the head and neck region. Promising results have been obtained with both groups of patients but these outcomes must be more rigorously evaluated in larger, possibly randomized clinical trials. Finally, we will summarize the critical issues that must be addressed if BNCT is to become a more widely established clinical modality for the treatment of those malignancies for which there currently are no good treatment options.
Figures

References
-
- Barth RF. Boron neutron capture therapy: a critical assessment. J Neurooncol. 2003;62:1–210. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
